

Beyond Omega-3 supplements: What PreventE4 Taught Us About Omega-3s and the Brain
Alzheimer’s prevention may depend on how the brain metabolizes omega-3s.

Happy Father’s Day to all the fathers, grandfathers, and families reading this.
Before discussing our recent trial, I want to thank the hundreds of research participants who made PreventE4 possible. This trial asked a lot of people: screening visits, blood draws, cognitive testing, MRI scans, study capsules, follow-up visits, and, for many, lumbar punctures twice. Prevention trials depend on people who are willing to contribute their time, often for the benefit of future generations. We are deeply grateful.
Should You Take DHA Supplements?
Many readers will come to this question first: Should I take a DHA or fish oil supplement for brain health?
PreventE4 does not give a simple yes or no answer.
It was a two-year prevention trial in cognitively healthy older adults at risk for dementia. That matters. Two years may be too short to detect whether a nutrient changes the long course of Alzheimer’s disease, especially before memory symptoms begin.
Whether someone chooses to take an omega-3 supplement is still a personal decision. We hope that the information gained from this trial will help you make that decision.
But the goal of PreventE4 was not only to answer whether people at risk of dementia should take DHA.
The deeper goal was to gain a better understanding of DHA biology and Alzheimer’s risk.
Why We Did PreventE4
DHA is an omega-3 fat that the brain needs.
It helps build brain cell membranes. It supports synapses, the connections between brain cells. It also helps regulate inflammation.
For years, studies have suggested that people with higher omega-3 levels tend to have better brain health.
From 1994 to 2008, my friend and mentor, Helena Chui, led the Aging Brain Study at USC. I joined that team later. In the Aging Brain Study, we found that cognitively healthy older adults with lower blood DHA had more amyloid on brain scans, smaller memory-related brain regions, and worse memory performance [1].
That finding was important, but it also showed the limits of observational studies.
When we see low DHA in the blood, it can mean at least two things.
It may mean a person is eating too little DHA, usually from fatty fish or other omega-3 sources.
Or it may mean the body or brain is breaking DHA down faster — what scientists call catabolism.
Both can also be true at the same time.
That distinction matters because a blood DHA level is not just a measure of intake. It may also be a clue about how the body and brain are handling DHA.
To answer this question we needed to do a DHA supplementation trial.
Why APOE4 Matters
APOE4 is the strongest common genetic risk factor for late-onset Alzheimer’s disease.
APOE is involved in moving lipids, or fats, around the brain. Since DHA is a brain lipid, we wondered whether APOE4 changes how DHA gets into the brain or how the brain uses it.
Earlier work suggested that APOE4 and Alzheimer’s disease stage may affect DHA delivery to the brain [2,3].
We conducted PET imaging with radiolabeled DHA to find more clues. Cognitively healthy APOE4 carriers showed higher DHA incorporation into gray matter, especially in the entorhinal cortex, a brain region affected early in Alzheimer’s disease [4].
One interpretation is that the APOE4 brain may be pulling in more DHA because it is using it faster, losing it faster, or trying to compensate for stress.
A later high-dose DHA pilot trial measured DHA in cerebrospinal fluid, or CSF, the fluid that surrounds the brain. DHA supplementation increased CSF DHA, but the increase was modest, and APOE4 carriers showed signals of lower omega-3 delivery than non-carriers [5].
Together, these studies led to PreventE4.
The question was simple: if we give enough DHA, can we get it into the central nervous system in people at risk, especially APOE4 carriers, before dementia begins?
Does the Form of DHA Matter?
Another common question is whether the form of DHA matters.
Some people argue that triglyceride-based DHA is the wrong form for brain delivery, and that phospholipid DHA would be superior. This is an important scientific question. Different DHA forms may behave differently.
But it is not correct to say that triglyceride DHA cannot enter phospholipid pools.
In our earlier pilot work, participants took triglyceride-based algal DHA. After supplementation, DHA increased not only in triglycerides, but also in phosphatidylcholine and cholesteryl ester lipid pools in both plasma and CSF [6]. These lipid pools appear to exchange with one another.
So the form of DHA may matter, but triglyceride DHA is not biologically isolated from phospholipid DHA. And they both reach the brain.
The Omega-3 Index
One practical way to measure omega-3 status is the omega-3 index.
This is the percentage of EPA plus DHA in red blood cell membranes. It is useful because red blood cells give a longer-term picture of omega-3 status than a single diet questionnaire.
Some brain health clinics now use the omega-3 index as part of a broader prevention workup [8], with a low or suboptimal index defined as < 6 and an optimal index>10. But these cut-offs are not validated in intervention trials.
The omega-3 index is not an Alzheimer’s test. A low number does not mean someone will develop dementia. And raising the number with supplements has not been proven to prevent cognitive decline.
It is best understood as one piece of a larger picture: diet, exercise, APOE genotype, vascular risk, inflammation, and brain biomarkers.
The Bigger Question: How Does the Brain Use DHA?
PreventE4 was designed to answer the delivery question and its implications on AD risk: once DHA reaches the brain, do we see signs of decreased AD risk?
This matters especially for APOE4.
In Alzheimer’s disease brain tissue, we see signs that polyunsaturated fatty acids are being broken down and remodeled in an inflammatory environment. This includes changes in omega-3 and omega-6 balance, lower DHA-related resolving mediators, and activation of inflammatory lipid pathways [9].
One enzyme that may be involved is cPLA2. This enzyme cuts fatty acids out of cell membranes. When it is overactive, it can release arachidonic acid and drive inflammatory lipid signaling.
In APOE4 and Alzheimer’s disease, we found that cPLA2 appears to be more active [9,14].
Put simply, the APOE4 brain may not only need more DHA delivered to it. It may also need help using DHA in the right way.
This is an important shift in thinking.
The question is not only: “How much omega-3 do you eat?”
It is also: “How does your brain metabolize omega-3s?”
What PreventE4 Was Designed to Test
I am deeply grateful to Lon Schneider for helping me design this trial. We had intense discussions on who we should recruit, what the outcomes should be, and how we interpret these findings. Wendy Mack was instrumental in planning and estimating sample sizes and analysis plans.
PreventE4 was a double-blind, placebo-controlled prevention trial in cognitively healthy older adults between ages 55 and 80 [10].
Participants had to have at least one dementia-related risk factor. These included obesity, high blood pressure, high cholesterol, low physical activity, or fewer than 12 years of education. They also had to have preserved daily function and no clinical dementia.
The trial intentionally looked for people with limited omega-3 intake. Participants were excluded if they were taking omega-3 supplements or consuming more than 200 mg per day of DHA [10].
In plain language, we were trying to find people who did not already eat much fish, had dementia risk factors, but did not yet have dementia.
That sounds straightforward.
It was not.
What It Took to Run the Trial
PreventE4 was conceived in 2016. Funding came in 2017 from NIH, two years after the application was submitted. This was followed by funding from ADDF. Recruitment began in May 2018.
The plan sounded simple: recruit cognitively healthy older adults with dementia risk factors, low omega-3 intake, and enough APOE4 carriers to test whether genotype changed DHA delivery.
In practice, it was enormously difficult.
We had to screen thousands of people to find the right participants. They had to be older adults who did not like to eat much fish, had dementia risk factors, were cognitively healthy, were willing to be followed for two years, and, in many cases, were willing to undergo a lumbar puncture.
This was especially challenging for APOE4 homozygotes, who are much less common than non-carriers or people with only one APOE4 copy.
The trial required constant outreach, prescreening, saliva collection, genotyping, phone calls, follow-up visits, and reassurance. Staff members worked tirelessly to call participants, answer questions, mail saliva kits, receive tubes, organize samples, and prepare batches for genotyping.
I remember the mechanics of it vividly.
Once a week, the genotyping workflow had to keep moving. I remember visiting the lab and finding packages dropped off by FedEx, sometimes many of them, waiting to be processed. On Fridays, I would pick up those packages and help deliver them to the genotyping team.
It was not glamorous work. It was not the part of science that people usually see. But without those tubes, labels, calls, packages, and staff members, there would be no PreventE4.
Then COVID changed everything.
Recruitment slowed. In-person visits became harder. Some participants dropped out. Safety rules changed how we could see people, collect samples, and keep the study moving. In 2021, the sample size had to be increased to account for the unexpected dropouts.
What began as a carefully powered prevention trial became a test of persistence.
Recruitment eventually ended in May 2024.
The Intervention
Participants were randomized to either 2 grams per day of DHA or an identical placebo for two years [10].
The DHA was algal-derived, which allowed a high, standardized dose.
Both the DHA and placebo groups also received a high-dose vitamin B complex. This was intentional. B-vitamin status and homocysteine metabolism can affect brain aging and may interact with omega-3 biology. By giving vitamin B supplementation to both groups, the trial reduced the chance that low B-vitamin status would confound the DHA results.
The primary outcome was measured at six months in the lumbar puncture subset. The question was whether DHA supplementation changed the ratio of DHA to arachidonic acid, or DHA/AA, in CSF [10].
CSF is not the brain itself. But it is one of the closest fluids we can safely measure in living people.
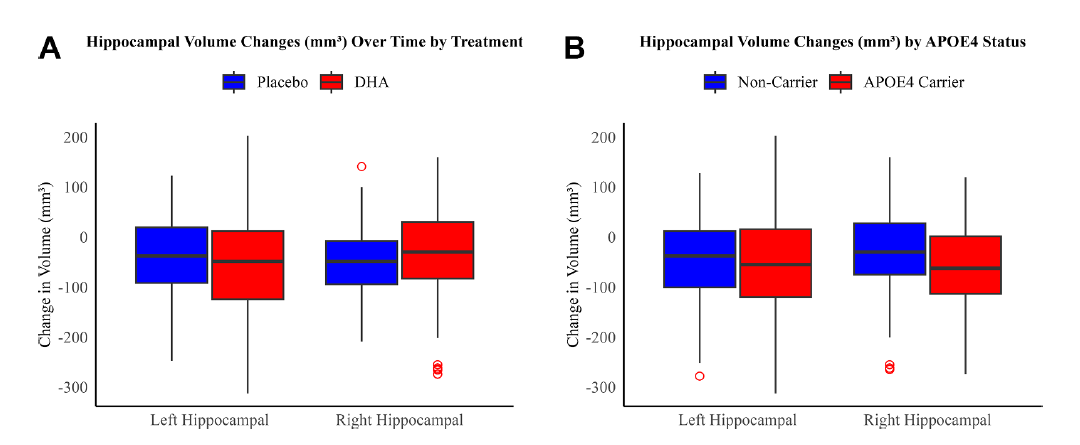
Secondary outcomes were measured over two years and focused on the brain. These included resting-state functional MRI, diffusion tensor imaging, and volumetric MRI [10]. In simpler terms, the trial asked whether DHA affected brain connectivity, white matter structure, hippocampal volume, and other imaging markers.
Exploratory outcomes included cognition, measured with the Repeatable Battery for the Assessment of Neuropsychological Status, or RBANS, along with blood biomarkers, inflammatory lipids, oxylipins, amyloid-related markers, phosphorylated tau, and microbiome sampling [10].
What We Found
The omega-3 index helped confirm that we recruited the right population and that the intervention did what it was supposed to do.
Testing showed that omega-3 levels in red blood cells climbed dramatically, from 4.9% to 11%. A 6% increase (shown in figure below)
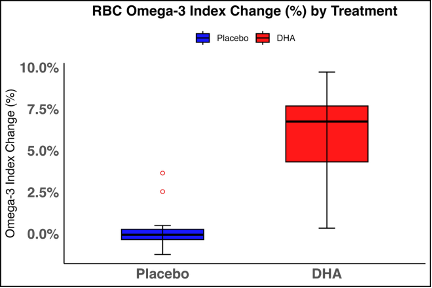
DHA levels in CSF, the fluid that surrounds the brain, rose by an average of 17% after six months [13].
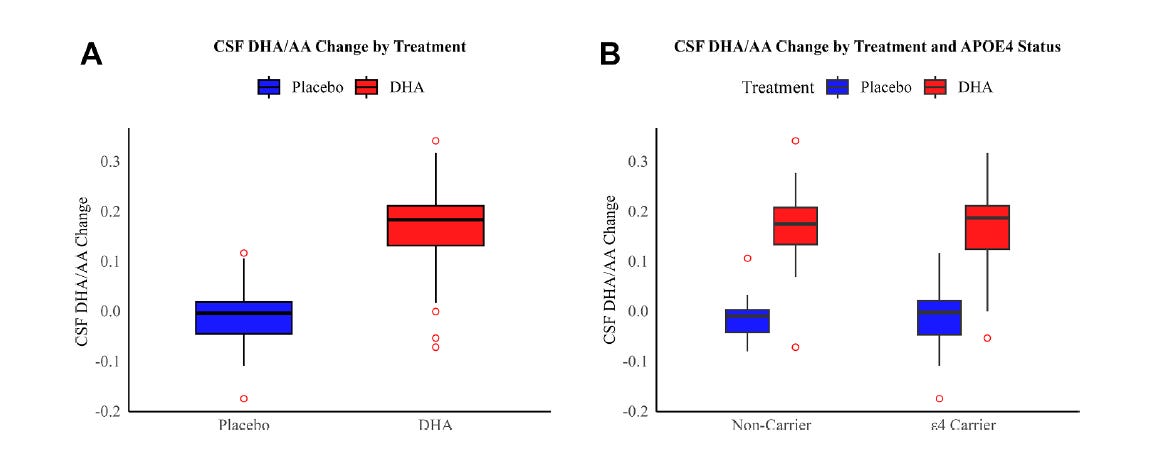
This confirmed that DHA reached its intended target.
The same increases were seen in people with an APOE4 gene, the group thought most likely to benefit from supplementation [13].
That finding matters.
At the level of the blood, people responded to DHA. The supplement was taken, absorbed, and incorporated into red blood cell membranes. At the level of CSF, DHA also increased.
So the simplest explanation is not that the dose failed to reach the body or the central nervous system.
But over two years, DHA supplementation did not improve cognition or slow hippocampal atrophy.
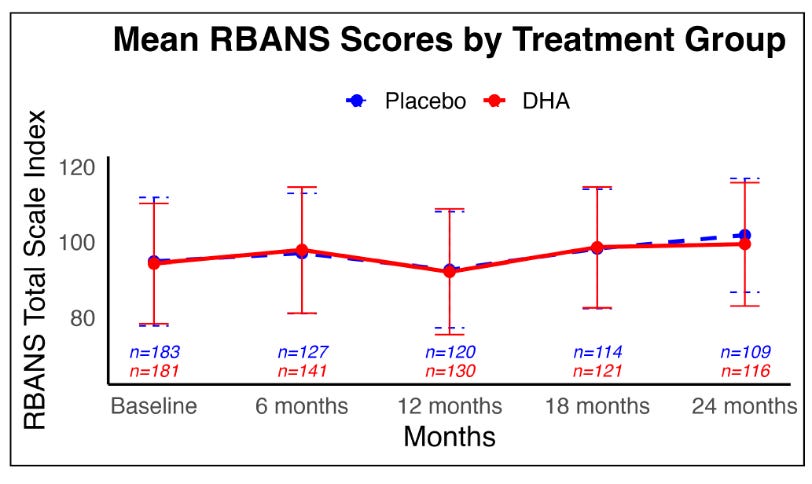
As you can see, there is a complete overlap between the treatment and placebo arms on cognition. No difference!
APOE4 carriers did show signs of greater vulnerability. They started slightly higher in the begining and learned less on the RBANS cognitive battery toward the end (Figure below). Something similar happened with hippocampal volumes. That finding is consistent with what we know about APOE4’s effect on cognition and hippocampal volume during preclinical (predementia) phases.
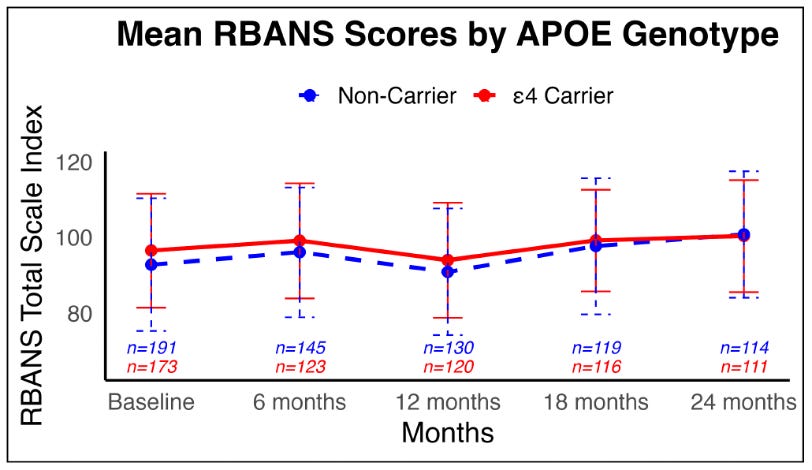
But being in the DHA treatment arm did not change that pattern.
This point is important.
Prevention trials in cognitively healthy people are hard because ceiling effects can make it difficult to detect change over only two years. But RBANS is a sensitive cognitive tool, and PreventE4 was a well-designed randomized trial. So while ceiling effects may have limited our ability to detect a small signal, we also have to be clear: we did not see a treatment signal on cognition or hippocampal volume.
Raising the omega-3 index to >10 did not affect AD biomarkers in 2 years. This is a real limitation to relying on the omega-3 index as an AD diagnostic.
That is the central result of PreventE4.
The intervention worked biologically. It changed omega-3 levels in blood and CSF. But it did not produce a measurable cognitive or hippocampal-volume benefit over two years in cognitively healthy older adults.
Why Prevention Trials Are So Hard
The first thing to remember is that PreventE4 was a prevention trial conducted in people without dementia.
That is both the strength and the challenge.
When people are cognitively normal at the start of a study, there may be very little room to improve on standard memory tests over only two years. This is called a ceiling effect. And participants do better on repeated testing. This is known as practice or learning effects. If a person is already doing well, a test may not be sensitive enough to show whether the brain is being protected.
Alzheimer’s disease also does not always progress in a straight line.
For years, changes may be slow and difficult to detect. Then, as someone approaches mild cognitive impairment or dementia, decline can accelerate.
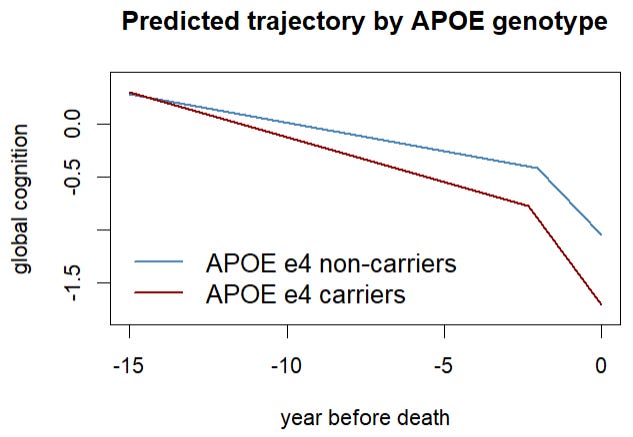
In other words, there may be two slopes: a slow early slope and a much steeper later slope (Figure above).
A two-year study in cognitively healthy people may happen during the slow slope, before standard cognitive tests or hippocampal volume show large treatment effects. But waiting until the steep slope begins may be too late, because neurodegeneration may be harder to reverse once neurons and synapses are already being lost.
That is the central dilemma of prevention research.
The best time to intervene may be before we can easily measure clinical decline.
Still, this limitation does not erase the finding. PreventE4 used sensitive cognitive testing, MRI measures, biomarkers, and a randomized placebo-controlled design, and APOE4 carriers had a signal that they learned less and had worse hippocampal volume changes. The study showed clear biological target engagement, but it did not show that DHA changed the cognitive or hippocampal-volume trajectory over two years.
Why We Tested One High Dose
One design decision is worth explaining.
We chose to test a high dose of DHA rather than several different doses.
That was intentional.
Since one of the central questions was whether APOE4 modifies DHA delivery and response, we chose a design that gave us the best chance of detecting that interaction.
With this dose, the biological signal was convincing. DHA increased in blood, and DHA increased in CSF, but we did not see an interaction with APOE4.
The effect of APOE4 on DHA brain transport is stronger in patients with mild cognitive impairment or dementia.
So the problem was not simply an inadequate dose or failed delivery at this clinical stage.
The harder question is what CSF DHA actually tells us.
CSF is not the same as a neuron. It is not a direct biopsy of a brain cell membrane. We cannot say with certainty that a rise in CSF DHA means the same rise occurred inside neurons or synapses.
But CSF is one of the best windows we have into the living human brain. It surrounds the brain and spinal cord, and changes in CSF often reflect changes in central nervous system biology. So while CSF DHA is not a perfect measure of neuronal DHA, it is a reasonable marker of brain delivery.
What This Means for Omega-3 Supplements
PreventE4 gives us a clearer way to think about omega-3s and brain health.
The message is not that omega-3s are unimportant. DHA is essential for the brain. It is part of neuronal membranes, synapses, and inflammatory signaling.
The message is also not that every person should or should not take a supplement. That decision is personal.
The more important lesson is that omega-3 supplementation alone is not a blunt solution for Alzheimer’s prevention.
A capsule cannot fully replace the biological context in which omega-3s seem to be most helpful.
In Mediterranean-style dietary patterns, omega-3s come with a broader lifestyle: fatty fish, vegetables, legumes, nuts, olive oil, physical activity, social connection, and lower cardiometabolic risk.
Whole foods bring more than one nutrient. Salmon contains DHA and EPA, but also protein, vitamin D, vitamin B12, selenium, potassium, and other nutrients. Walnuts and seeds provide plant-based omega-3s along with fiber, minerals, and polyphenols.
That context may matter as much as the omega-3 number itself.
It is plausible that a healthy lifestyle does more than raise omega-3 levels. It may also create the biology needed to use DHA effectively.
A person who eats fatty fish, exercises, sleeps well, has good vascular health, and has lower chronic inflammation may not only have higher omega-3 levels. They may also have a brain environment that transports, retains, remodels, and uses DHA better.
That is different from taking a capsule in the setting of poor sleep, high stress, sedentary behavior, obesity, insulin resistance, and an ultraprocessed diet.
In that setting, DHA may reach the blood and even the central nervous system, but the broader biology may not be ready to use it effectively.
This is the key shift.
Omega-3s are not magic. They are part of a biological system. And a quick fix with supplements may not work.
Where We Go Next
PreventE4 did not end the omega-3 story. It sharpened the next question.
The problem may not simply be getting DHA into the body or even into CSF during preclinical AD. The problem may be whether the brain can retain, remodel, and use omega-3s in the right way.
This is why we think the next generation of research needs to focus on DHA metabolism.
How does inflammation change brain DHA use? What is the role of gut dysbiosis?
And can we change the brain environment so omega-3s work better?
This is where lifestyle becomes important.
A healthy lifestyle may not only raise omega-3 levels. It may also create the biology needed to use DHA effectively. A person who eats fatty fish, exercises, sleeps well, has good vascular health, and has lower chronic inflammation may have a brain environment that transports, retains, remodels, and uses DHA better.
That may be more meaningful than any single omega-3 index number, supplement label, or blood level.
This is also where our work on brain-penetrant cPLA2 inhibitors comes in.
cPLA2 is an enzyme that cuts polyunsaturated fatty acids out of cell membranes. When it is overactive, it can release both arachidonic acid and DHA and drive unresolved inflammation. In APOE4 and Alzheimer’s disease, cPLA2 appears to be more active. That may push the brain toward a state where polyunsaturated fatty acids are being broken down, remodeled, or consumed faster than they can be used for healthy membrane repair and anti-inflammatory signaling [9,14].
In simple terms, giving DHA may not be enough if the brain is stuck in a lipid-inflammatory state that keeps burning through these fats.
Our future direction is to target that biology directly.
We are developing brain-penetrant cPLA2 inhibitors designed to reduce harmful inflammatory lipid signaling and help restore a healthier omega-6 to omega-3 balance in the brain. The goal is not to replace omega-3 nutrition. The goal is to change the brain environment so omega-3s can be used more effectively [14].
That is still early-stage work. It is not yet a human Alzheimer’s treatment.
That is where nutrition, lipid biology, neuroinflammation, lifestyle, and drug discovery now come together.
Take-Home Messages
PreventE4 does not give a simple yes or no answer about whether an individual should take DHA supplements.
The trial showed that high-dose DHA reached its biological targets: omega-3 levels in red blood cells rose from 4.9% to 11%, and CSF DHA rose by about 17%.
The same biological response was seen in APOE4 carriers.
DHA did not improve cognition or slow hippocampal atrophy over two years.
APOE4 carriers learned less on RBANS and had greater hippocampal atrophy, but DHA treatment did not change that pattern.
That does not mean omega-3 biology is unimportant. It means delivery alone may not be enough.
The next question is DHA metabolism: how the brain transports, retains, remodels, and uses omega-3s.
A holistic lifestyle may help create the biology needed to use DHA effectively.
Future prevention may require combining nutrition, lifestyle, biomarkers, and therapies that target inflammatory lipid metabolism, including cPLA2.
Publication
Yassine HN, Ghasem Pour S, Juarez M, Arellanes IC, Ali N, Dikeman D, Sanchez A, Park J, Kerman B, Duro MV, Asante I, Louie S, Kono N, D’Orazio L, Chui H, Mack WJ, Harrington MG, Braskie MN, Schneider LS.
CNS Target Engagement of High-dose DHA Supplementation in Older Adults at Risk for Dementia: A Randomised, Double-blind, Placebo-controlled Trial.
Acknowledgments
PreventE4 was a team effort. Hussein N. Yassine designed and supervised the trial, obtained funding, and wrote the manuscript. Sara Ghasem Pour helped with data analysis and manuscript drafting. Nada Ali assisted with manuscript drafting. Marlene Juarez helped with cognitive testing. Isabella C. Arellanes and Dante Dikeman coordinated study visits. Ashley Sanchez assisted with blood sample collection and storage. Bilal Kerman, Marlon V. Duro, and Isaac Asante assisted with biomarker measurements. Stan Louie supervised biomarker management. Jackson Park assisted with study coordination. Naoko Kono led data management. Lina D’Orazio supervised cognitive testing. Helena Chui helped with study design. Wendy J. Mack supervised study design and all data analysis. Michael G. Harrington performed lumbar punctures. Meredith N. Braskie oversaw the imaging biomarkers. Lon S. Schneider supervised study design, grant applications, and manuscript writing. Naoko Kono and Wendy J. Mack accessed and verified the underlying data. All authors read and approved the final version of the manuscript.
This study was funded in part by the National Institutes of Health/National Institute on Aging, including RF1AG076124, R01AG055770, R01AG067063, R01AG054434, R21AG056518, and P30AG066530 to Hussein N. Yassine; the Alzheimer’s Drug Discovery Foundation, GC-201711–2014197 to Hussein N. Yassine and Lon S Schneider; and donations from the Vranos and Tiny Foundations and Ms. Lynne Nauss to Hussein N. Yassine. Wendy J. Mack, Meredith N. Braskie, and Lon S. Schneider also received funding from NIH R01AG054434 and the Alzheimer’s Drug Discovery Foundation. We also thank the members of the Data and Safety Monitoring Board for their oversight and guidance.
References
Yassine HN, Feng Q, Azizkhanian I, et al. Association of serum docosahexaenoic acid with cerebral amyloidosis. JAMA Neurology. 2016.
Yassine HN, Rawat V, Mack WJ, et al. The effect of APOE genotype on the delivery of DHA to cerebrospinal fluid in Alzheimer’s disease. Alzheimer’s Research & Therapy. 2016;8:25.
Yassine HN, Braskie MN, Mack WJ, et al. Association of docosahexaenoic acid supplementation with Alzheimer disease stage in apolipoprotein E ε4 carriers: a review. JAMA Neurology. 2017;74(3):339–347.
Yassine HN, Croteau E, Rawat V, et al. DHA brain uptake and APOE4 status: a PET study with [1-¹¹C]-DHA. Alzheimer’s Research & Therapy. 2017;9:23.
Arellanes IC, Choe N, Solomon V, et al. Brain delivery of supplemental docosahexaenoic acid (DHA): a randomized placebo-controlled clinical trial. EBioMedicine. 2020;59:102883.
Bantugan MA, Xian H, Solomon V, et al. Associations of ApoE4 status and DHA supplementation on plasma and CSF lipid profiles and entorhinal cortex thickness. Journal of Lipid Research. 2023;64(6):100354. doi:10.1016/j.jlr.2023.100354.
Yassine HN, Samieri C, Livingston G, et al. Nutrition state of science and dementia prevention: recommendations of the Nutrition for Dementia Prevention Working Group. The Lancet Healthy Longevity. 2022;3:e501–e512.
Yassine HN. The omega-3 index in Alzheimer’s disease: ready for prime time? American Journal of Clinical Nutrition. 2022.
Ebright B, Assante I, Poblete RA, et al. Eicosanoid lipidome activation in post-mortem brain tissues of individuals with APOE4 and Alzheimer’s dementia. Alzheimer’s Research & Therapy. 2022;14:152.
Yassine HN, Arellanes IC, Mazmanian A, et al. Baseline findings of PreventE4: a double-blind placebo controlled clinical trial testing high dose DHA in APOE4 carriers before the onset of dementia. Journal of Prevention of Alzheimer’s Disease. 2023.
Yassine HN, Carrasco AS, Badie DS. Designing newer omega-3 supplementation trials for cognitive outcomes: a systematic review guided analysis. Journal of Alzheimer’s Disease. 2024.
Ebright B, Duro MV, Chen K, Louie S, Yassine HN. Effects of APOE4 on omega-3 brain metabolism across the lifespan. Trends in Endocrinology & Metabolism. 2024.
Yassine HN, Ghasem Pour S, Juarez M, et al. CNS target engagement of high-dose DHA supplementation in older adults at risk for dementia: a randomized, double-blind, placebo-controlled trial. EBioMedicine. 2026.
Sadybekov AV, Duro MV, Wang S, et al. Development of potent, selective cPLA2 inhibitors for targeting neuroinflammation in Alzheimer’s disease and other neurodegenerative disorders. npj Drug Discovery. 2026.
We would have seen that signal of harm in controlled trials. We don't see harm or benefit. But that does not mean at an individual level some may benefit and others may develop side effects.
Wow, I found your substack after reading the Skeptical Cardiologist. Love this breakdown of your study. Appreciate how you explain the findings. Looking forward to reading more of your work.