

Are the New Alzheimer's Drugs Really "Disease-Modifying"?
What the evidence supports about lecanemab and donanemab — and what it does not.

The arrival of anti-amyloid therapies has revived the field of Alzheimer’s disease, but whether they truly qualify as disease-modifying remains an open and unresolved question.
This post is the summary of a discussion with my friend and mentor, Lon Schneider, whose work on Alzheimer’s trials has shaped my interpretation of AD clinical trial readouts.
To get a better understanding of the background of this post, I suggest you take a look at two past posts:
1. Where does amyloid fit in the pathogenesis of AD?
2. How do we interpret blood amyloid biomarkers?
In 2023, the U.S. Food and Drug Administration approved a new drug for early Alzheimer’s disease called lecanemab (sold as Leqembi). A second drug, donanemab (Kisunla), followed in 2024. Both are antibodies — proteins made in a lab and given by IV — designed to clear amyloid, the sticky protein that builds up in Alzheimer’s brains. Some regulators and drugmakers describe them as “disease-modifying.”
Their arrival is the first significant progress in Alzheimer’s drug development in decades. After many years of failed trials, these are the first treatments to clear amyloid from patients’ brains and to produce statistically significant benefits on composite, cognitive, and daily-living measures in large Phase 3 studies, and on core AD biomarkers. Those results justified FDA approval and are not in dispute.
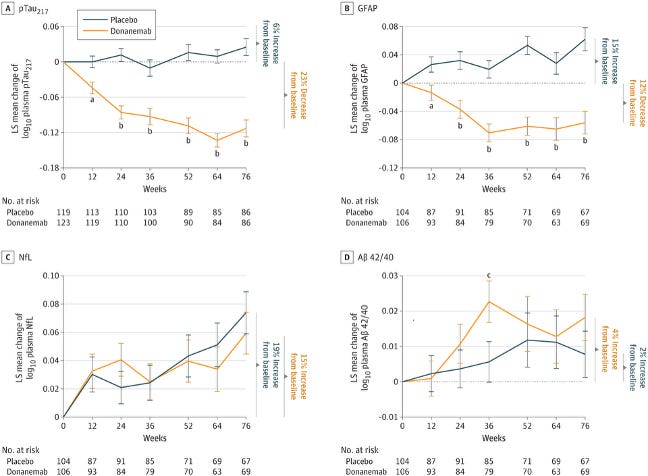
Figure 1. Changes in plasma Alzheimer’s disease biomarkers with donanemab treatment.
Least-squares mean (±SE) change from baseline over 76 weeks in (A) plasma p-tau217, (B) GFAP, (C) neurofilament light chain (NfL), and (D) Aβ42/40 ratio in patients receiving donanemab versus placebo. Donanemab treatment is associated with sustained reductions in p-tau217 and GFAP, stabilization of NfL compared with placebo, and an increase in the Aβ42/40 ratio, consistent with amyloid clearance. Numbers at risk are shown below each panel.
The “disease-modifying” label, though, sets a higher bar than the trial evidence has yet met. By the European Medicines Agency’s standard, a disease-modifying drug has to do more than help while you’re taking it — it has to actually change the course of the illness. No anti-amyloid antibody has been shown to do that in a trial designed to test it. Most data so far support that these drugs may modestly reduce symptoms while patients receive them.
After 18 months, patients on lecanemab or donanemab decline a little less than placebo patients on tests of memory and daily function. The difference is real and statistically reliable — but statistical reliability isn’t the same as a noticeable change, and a measurable difference on a test isn’t the same as a meaningful change in the disease.
What “disease-modifying” actually means
A 2017 paper by my colleague Dr. Jeffrey Cummings offered a framework for evaluating disease-modifying therapies (DMT) in Alzheimer’s. It uses the “slope of decline” to separate drugs that truly slow the disease from those that only ease symptoms.

Figure 2 above (adapted from Cummings, J. (2017). JPAD) illustrates one framework for how a disease-modifying treatment (DMT) can change the trajectory of Alzheimer’s.
The Solid Line: The typical path of the disease, with memory and thinking declining steadily over time. The arrow marks DMT initiation — when a treatment that targets the biology of the disease begins.
The Dashed Line: The goal of treatment is to slow the rate of decline so a person keeps their independence and cognitive health longer.
The European Medicines Agency — Europe’s drug regulator — has since set out a clear working standard. A symptomatic drug helps you while you take it; stop it, and the benefit fades. A disease-modifying drug actually changes the disease, so that people who took it remain better off even after stopping. The disease has been put on a different track.
To prove this, regulators look for specific trial designs — typically ones in which some patients start on a placebo and are later switched to the active drug. If the late-starters never catch up, the early treatment must have changed something durable. If they do catch up, the drug was probably just helping with symptoms while it was being given.
This “slope separation” picture above is a useful starting point, but on its own it doesn’t meet the EMA’s bar. The agency expects a real slowing of clinical decline alongside a matching change in biological markers like amyloid or tau. It also asks that the slowing be meaningful in patients’ daily lives, not just on a graph — and that it reflect a true shift in the disease, not an ongoing symptomatic effect. That is why regulators favor “delayed-start” or “withdrawal” designs over simple slope comparisons.
An example of a delayed start is shown in Figure 3 below:

Early Starters: Patients who start the active treatment on day one.
Late Starters: Patients who start on a placebo and switch to active treatment after a set period.
The Outcome: If late starters never catch up, the drug likely slows the disease itself rather than just masking symptoms.
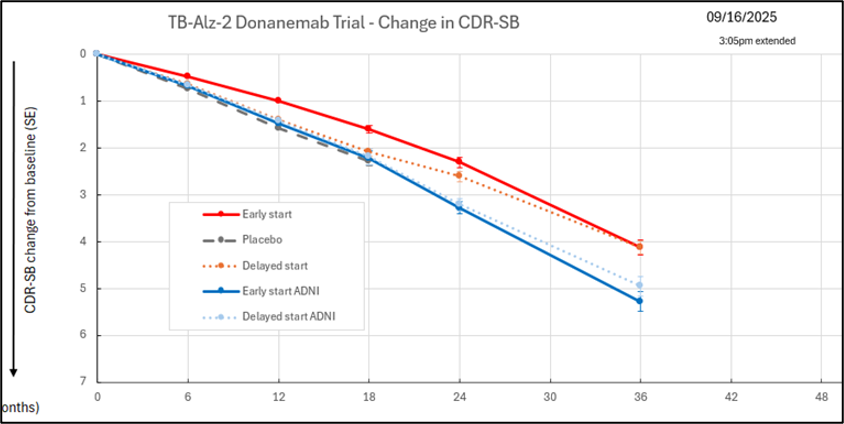
In the TRAILBLAZER-ALZ 2 donanemab trial, the delayed-start and early-start groups appear to converge over time, Figure 4 (Modified from Mintun MA. Donanemab TRAILBLAZER-ALZ in Early Symptomatic Alzheimer’s Disease: Efficacy and Safety from the Long-Term Extension. Presented at: 2023 International Conference on Alzheimer’s and Parkinson’s Diseases (AD/PD); March 28–April 1, 2023; Gothenburg, Sweden. Eli Lilly and Company, Indianapolis, IN. Available from Eli Lilly medical materials.
“Time Saved” Does Not Mean the Disease Is Changed
Another framing of the benefit is “time saved” (see figure 5 below). It describes a delay in reaching a given level of symptoms — not a fundamental change in the disease itself. “Time saved” only reflects true disease modification if the benefit persists after treatment stops, or if the trajectory is permanently changed. Current studies have shown neither. So while the phrase sounds meaningful, it may simply represent a temporary slowing of symptoms.
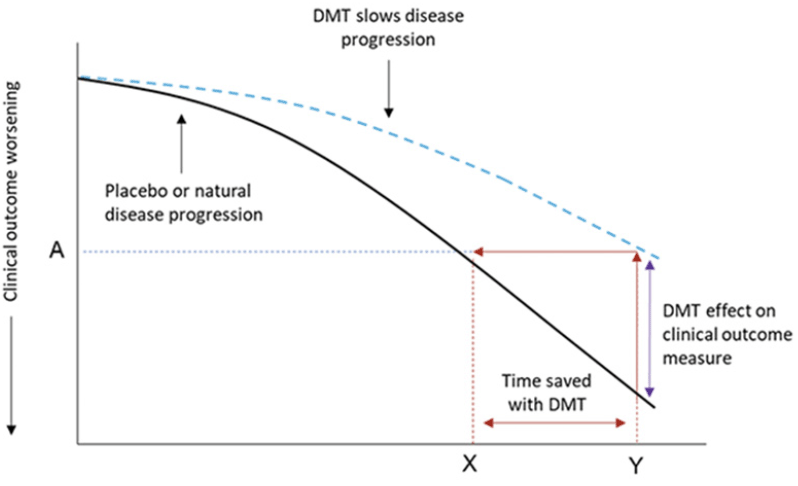
Adapted from Dickson SP, et al. Time saved as a demonstration of clinical meaningfulness and illustrated using the donanemab TRAILBLAZER-ALZ study findings. Journal of Prevention of Alzheimer’s Disease, 2023
What the drugs appear to do
Two things show up consistently in the trials.
First, the drugs clear amyloid from the brain. PET scans confirm that plaques drop, often back to normal levels, and other markers of brain damage — including the protein tau — also move in the expected direction.
Second, after 18 months, patients on the drug score slightly better than patients on placebo on standard tests of memory, thinking, and daily activities. The relative slowing of decline is roughly 25 to 30 percent. Supporters frame this as about seven to eight extra months in the milder stages of disease, with simulation models projecting up to two and a half years if the slowing keeps compounding. “Time saved” is one framing that patients and families may likely hear from a doctor.
Two cautions about that framing.
First, the absolute differences on the tests are small. On the cognitive test most often used (ADAS-Cog, 0–70), the average difference between groups was less than one point. On a common dementia severity scale (CDR-SB, 0–18), it was about a third of a point. Most clinicians say a patient or family wouldn’t notice anything smaller than 2–4 points on the cognitive test or 1–2 points on the dementia scale — the trial differences fall below those thresholds. A 2026 Cochrane review pooling 17 trials and more than 20,000 patients called the effect on memory and thinking “trivial.”
Second, the “time saved” calculation only really makes sense if the slowing is true disease modification. If a patient takes lecanemab for two years, comes out a bit ahead on cognitive testing, and then stops — does the gap hold, close, or grow? The answer determines whether “time saved” is a real bank balance or a temporary read on the meter. We don’t yet have one.
Why the disease-modifying claim outruns the data
Two further problems push the other way.
First, the trials weren’t set up to test it. After CLARITY AD ended, all participants were offered the active drug in an open-label extension. The manufacturer has used that follow-up to argue that the benefit accumulates over three years, and the placebo group never catches up. A 2026 commentary coming out soon in Alzheimer’s & Dementia points out that the statistical analysis needed to support this claim was never done; the argument relies on visual separation in figures rather than formal modeling.
Second, where the analysis has been done, it points the other way. In the 36-month donanemab data, the placebo-then-treated group catches up to the early-treated group — the pattern of a symptomatic drug. And in the DIAN-TU trial, in people with rare genetic forms of Alzheimer’s caused unambiguously by amyloid, treatment cleared amyloid but produced no clinical benefit over nearly five years.
A useful comparison: cholinesterase inhibitors
For more than two decades, an older class of Alzheimer’s drugs — cholinesterase inhibitors taken as daily pills (donepezil, rivastigmine, galantamine) — has been used to treat the disease. These have always been called “symptomatic”: they help while they’re taken but don’t change the underlying disease.
A recent analysis across more than 40 trials compared the older pills with the newer antibodies. On the same tests of memory and daily function, the two classes produce similar effects — on some measures, the older pills produce slightly larger differences.
A 2026 study in The Lancet Regional Health – Europe found that patients who stayed on cholinesterase inhibitors for four years were nearly two points ahead on a standard cognitive test (the MMSE) compared with patients who stopped. By the same reasoning used to argue lecanemab is disease-modifying, that sustained benefit would also count — yet no one calls cholinesterase inhibitors disease-modifying.
This isn’t to say the two classes are interchangeable. The biology differs. Cholinesterase inhibitors boost acetylcholine, a brain chemical that supports memory and thinking; they ease symptoms but don’t touch amyloid, tau, or the underlying pathology. The anti-amyloid antibodies clear amyloid from the brain and lower tau biomarkers in blood and spinal fluid. That biological effect is unprecedented in Alzheimer’s care, and it is the foundation for regulatory approval. The unsettled question — the one ongoing trials are designed to answer — is whether that biological change will translate into a durable, disease-modifying clinical benefit. On the scales that matter for patients and families today, the two classes still look similar in size of effect, even though the underlying biology is different.
What could resolve this
Two ongoing trials are worth watching.
The first is TRAILBLAZER-ALZ 3, testing donanemab in people who don’t yet have Alzheimer’s symptoms but whose brain scans show elevated amyloid. The endpoint is whether participants reach a clinical diagnosis over roughly three and a half years. Because the trial measures whether disease itself emerges, a positive result would be hard to explain as merely symptomatic — and the disease-modifying claim would become much stronger. A negative result would be a serious blow to the amyloid hypothesis as a basis for prevention.
AHEAD 3-45 is a similar prevention trial of lecanemab. It is important, but on its own, it cannot prove disease modification — even a statistically significant cognitive benefit could be explained as a temporary effect.
Trials combining anti-amyloid drugs with treatments targeting tau or brain inflammation are also underway. Larger and more durable effects from those combinations would strengthen the case for amyloid as part of a disease-modifying strategy.
Take-home messages
FDA approval rests on Phase 3 trials showing statistically significant benefits on composite, cognitive, and daily-living measures at 18 months. After decades of failed Alzheimer’s trials, that is real progress.
By Europe’s regulatory standard, however, no anti-amyloid antibody has yet been formally shown to be disease-modifying — that is, to change the underlying course of the illness. The 18-month evidence is consistent with a symptomatic effect; ongoing trials may shift that picture.
The differences favoring treatment are real but small in absolute terms — below what many clinicians consider noticeable on standard scales.
Advocates frame the benefit as “time saved” — months of additional independence. That framing only fully holds if the slowing is durable, which hasn’t yet been demonstrated.
The antibodies differ biologically from older cholinesterase inhibitors: they clear amyloid and lower tau, while the older drugs don’t touch this pathology. Whether that biological difference translates into a durable disease-modifying clinical benefit is the central open question.
Costs and risks are real: about 1 in 8 treated patients develops brain swelling or microbleeds, and treatment requires IV infusions, repeat MRIs, genetic testing, and around $26,000 a year.
Even if current evidence does not yet meet strict definitions of disease modification, anti-amyloid antibodies represent progress: they show that targeting a biological feature associated with Alzheimer’s disease can translate into consistent, measurable slowing of clinical decline in large trials.
The TRAILBLAZER-ALZ 3 prevention trial of donanemab could potentially settle the disease-modifying question over the next few years.
Decisions about starting, continuing, or stopping treatment are personal, best made with a clinician who can weigh the evidence, costs, and individual circumstances. Nothing here, on its own, is a reason to stop a treatment that is working for someone.
Sources
European Medicines Agency. Guideline on the clinical investigation of medicines for the treatment of Alzheimer’s disease (CPMP/EWP/553/95 Rev. 2). 2018.
Cummings, J. (2017). “Defining Disease Modifying Therapy for Alzheimer’s Disease.” The Journal of Prevention of Alzheimer’s Disease, 4(2), 109–115. doi.org.
Aisen P, Bateman RJ, Crowther D, et al. The case for regulatory approval of amyloid-lowering immunotherapies in Alzheimer’s disease based on clearcut biomarker evidence. Alzheimer’s & Dementia 2025;21:e14342.
Cummings J. Anti-amyloid monoclonal antibodies are transformative treatments that redefine Alzheimer’s disease therapeutics. Drugs 2023;83:569–576.
Nonino F, Minozzi S, Sambati L, et al. Amyloid-beta-targeting monoclonal antibodies for people with mild cognitive impairment or mild dementia due to Alzheimer’s disease. Cochrane Database of Systematic Reviews 2026, Issue 4: CD016297.
Schneider LS, Kennedy RE, Cutter G. Caution in interpreting disease-modification claims with lecanemab: selective reporting and causal inference. Alzheimer’s & Dementia 2026 (Letter to the Editor).
The Lancet Neurology. Stopping Alzheimer’s disease before symptoms start [Editorial]. Lancet Neurology 2026;25:213.
Giacobini E, Schneider LS. Cholinesterase inhibitors and amyloid-targeting antibody treatments show similar clinical effect. Presented at ADPD, Copenhagen, March 2026.
Lecerf S, Guinebretiere O, Bentegeac R, et al. The Lancet Regional Health – Europe 2026;62.
Dickson SP, et al. Time saved as a demonstration of clinical meaningfulness and illustrated using the donanemab TRAILBLAZER-ALZ study findings. Journal of Prevention of Alzheimer’s Disease, JPAD 2023.
Such a thoughtful discussion addressing one of the central tensions in modern neurology: how to interpret modest clinical effects in devastating diseases where patients and families are understandably desperate for progress. What I appreciated most is that the article moved beyond simplistic “breakthrough” versus “failure” narratives and instead examined the Alzheimer’s drug landscape with nuance, particularly around endpoints, risk-benefit balance, and mechanistic assumptions. One of the most important points is the distinction between altering a biomarker and meaningfully altering lived cognitive outcomes. The newer anti-amyloid therapies clearly demonstrate that amyloid plaques can be reduced in the human brain, which is scientifically significant. But the larger clinical question is whether plaque reduction translates into substantial preservation of memory, independence, executive function, and quality of life over meaningful time horizons. That gap between biologic effect and functional outcome is where much of the debate appropriately centers. I also appreciated the broader implication that Alzheimer’s disease is probably far more biologically complex than amyloid accumulation alone. Neuroinflammation, vascular dysfunction, insulin resistance, mitochondrial impairment, sleep disruption, immune signaling, synaptic loss, tau pathology, and metabolic aging likely interact over decades before symptoms emerge. The field increasingly feels less like a single-pathway disease model and more like a systems-level neurodegenerative process. At the same time, I think it is important not to dismiss incremental progress simply because it is imperfect. Neurology historically has had relatively few disease-modifying therapies for neurodegeneration, so even modest slowing of decline may matter deeply for patients and families depending on disease stage and risk tolerance. The challenge is communicating those benefits honestly without overstating them, especially given the risks of ARIA (amyloid-related imaging abnormalities), cost considerations, monitoring burden, and unequal access to advanced treatment infrastructure. What I find especially interesting is how these therapies may ultimately reshape the timing of intervention more than late-stage treatment itself. If Alzheimer’s pathology begins decades before cognitive symptoms, the future may depend increasingly on identifying high-risk individuals earlier through genetics, blood biomarkers, retinal imaging, sleep analysis, and longitudinal metabolic profiling rather than waiting for overt impairment. Overall, I believe this piece captured the complexity of the current moment in Alzheimer’s research very well: genuine scientific progress coexisting with important unanswered questions about causality, clinical significance, accessibility, and what successful brain aging prevention will ultimately require. Thanks again for sharing!
The cholinesterase inhibitor comparison reframes the whole discussion in a way that's hard to ignore. The biology clearly differs, but the measurable outcomes don't, at least not yet. Excellent breakdown, Hussein!