

Of Mice and Men: The Rapamycin Problem in Alzheimer’s Prevention
Insights from tissue specific immune aging biomarkers

A friend recently asked me a personal question.
She carries a genetic risk for Alzheimer’s disease and wanted to know whether she should take rapamycin to reduce her risk.
This post is dedicated to her.
My answer today is: no.
Not because rapamycin is uninteresting. It is one of the most important drugs in aging biology. It extends lifespan in mice, affects a major growth-and-repair pathway, and may improve some aspects of immune function in older adults.
But the human evidence does not show that rapamycin works in people the way it works in mice.
We do not yet have convincing evidence that rapamycin slows human aging, improves Alzheimer’s biomarkers, prevents cognitive decline, or reduces dementia risk. The strongest human data are much narrower: vaccine response, infection-related outcomes, and tissue-specific markers such as skin aging.
That is not enough to justify taking rapamycin today for Alzheimer’s prevention. But it gets more complicated. How do we know it’s working for aging or AD?
What Is Rapamycin?
Rapamycin, also called sirolimus, is a drug originally discovered from bacteria found on Easter Island, also known as Rapa Nui.
It blocks part of a pathway called mTOR, short for mammalian target of rapamycin.
Think of mTOR as one of the cell’s main growth switches. When food and energy are plentiful, mTOR tells cells to grow, build proteins, divide, and store nutrients. When mTOR activity goes down, cells may shift more toward repair, recycling, and maintenance.
This is why rapamycin became so interesting to aging researchers.
Aging is not only about time passing. It is also about how cells handle damage, inflammation, protein buildup, and repair. By lowering mTOR activity, rapamycin may push cells away from constant growth and toward cellular maintenance.
But this does not mean that “slowing metabolism” automatically slows aging.
That is too simple.
A better way to think about rapamycin is that it changes the balance between growth mode and repair mode. That may help in some tissues, at some ages, and in some disease states. But growth signals are also needed for muscle repair, wound healing, immune defense, and recovery after exercise.
The real question is not whether mTOR is good or bad.
The real question is: how much mTOR activity, in which tissue, at what age, and at what time?
Why Rapamycin Became Famous
The strongest evidence for rapamycin comes from mice.
The landmark study was published in 2009 through the National Institute on Aging’s Interventions Testing Program, or ITP.
This was not a small mouse experiment. It was a large, multi-site study using genetically diverse mice. More than 1,900 mice were included. Rapamycin treatment began late in life, at about 20 months of age.
The result was striking: rapamycin extended lifespan in both male and female mice.
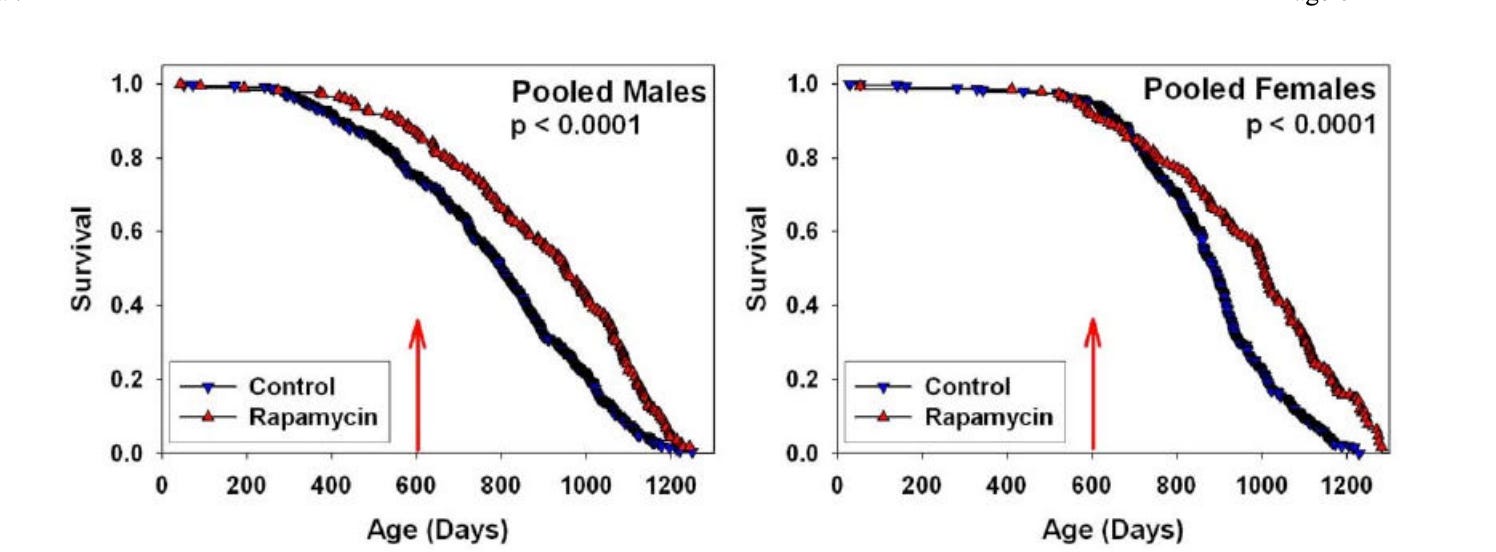
Figure 1: from Harrison et al. 2009 — t rapamycin extended lifespan in genetically heterogeneous mice when started late in life
One way the investigators reported this was by examining the age at which 90% of the mice had died. That age increased from about 1,078 to 1,179 days in males, and from about 1,094 to 1,245 days in females.
This mattered because the drug worked even when started late in life. That suggested rapamycin might affect the biology of aging itself, not just growth or development.
Later mouse studies supported the same general idea. Rapamycin became one of the most reproducible lifespan-extending drugs in mice. But those studies also showed that the effect depends on dose, sex, timing, and treatment schedule.
That is impressive.
But mouse lifespan extension is not the same as human disease prevention.
Rapamycin and Alzheimer’s Mouse Models
Rapamycin has also been tested in Alzheimer’s mouse models.
In some models, including 3xTg-AD mice, rapamycin or mTOR inhibition has been reported to reduce amyloid and tau-related pathology and improve memory-like performance.
The mechanism makes sense.
mTOR inhibition can increase autophagy, the cell’s recycling system. Autophagy helps cells clear damaged proteins and worn-out cell parts. Since Alzheimer’s disease involves protein buildup and cellular stress, improving cleanup is an attractive idea.
But Alzheimer’s mouse models are not the same as human Alzheimer’s disease.
They are simplified versions of the disease. Many are engineered to develop amyloid or tau changes quickly. Human Alzheimer’s develops over decades and is shaped by aging, blood vessels, sleep, infections, metabolism, immune history, and genetics such as APOE4.
So the mouse studies are useful for understanding possible mechanisms.
They are not proof that rapamycin prevents Alzheimer’s disease in humans.
Why Mice Are Not Small Humans
The mouse data justify human trials.
They do not justify routine human use.
Mice and humans age differently. Mice are short-lived and fast-growing. Humans grow slowly and live for decades. A drug that slows a growth pathway in a mouse may not have the same effect in a long-lived human.
Laboratory mice also live in controlled environments. Their food, movement, temperature, and exposure to germs are carefully managed.
Humans live in the real world.
We experience infections, stress, poor sleep, medications, injuries, exercise, obesity, diabetes, dental disease, and decades of immune memory.
This matters especially for the immune system.
By older age, each person has a unique immune biography. One person may have had shingles, repeated respiratory infections, autoimmune disease, insulin resistance, or chronic inflammation. Another person may not.
So two 70-year-olds may have very different immune systems.
If rapamycin helps one kind of immune aging, it may not help another. It may even hurt some people if the dose, timing, or baseline biology is wrong.
That is why biomarkers matter. And for immune aging, we are learning that they need to be tissue or organ-specific.
In mice, we can give rapamycin and measure lifespan. In humans, we need to know what biology we are trying to improve.
Is it high mTOR activity? Poor vaccine response? Chronic inflammation? Weak autophagy? Senescent cells? Metabolic dysfunction? Brain inflammation?
Right now, we do not have a simple clinical test that answers this.
How Can Rapamycin Improve Immunity?
Rapamycin can seem confusing.
At high or continuous doses, it can suppress the immune system. That is why rapamycin and related drugs have been used in transplant medicine.
But low-dose or intermittent mTOR inhibition may act differently, especially in older adults.
Older immune cells may be chronically stimulated, inflamed, and inefficient. They may be “on” all the time, but not very good at responding to a new threat.
A short course of mTOR inhibition may reduce some of that background noise. It may help immune cells clean up damaged parts and respond more effectively to a challenge, such as a vaccine.
So rapamycin may not “boost” immunity like pressing the gas pedal.
It may help some older immune cells respond more cleanly by taking them out of a stressed, inefficient, or exhausted state. I have dedicated a previous post to why immune exhaustion is a hot topic in AD.
That is the idea behind the vaccine-response studies, and why it may be relevant for the brain. But we still cannot link them.
What Do Human Studies Show?
Human studies of rapamycin and rapamycin-like drugs do exist. They are interesting, but limited.
Mannick 2014: Vaccine Response
The best-known positive human study was published by Mannick and colleagues in 2014.
This randomized trial tested RAD001, also called everolimus, a rapamycin-like drug, in older adults before influenza vaccination. Participants received short-term treatment before vaccination. The main outcome was antibody response to the flu vaccine.
The result was encouraging: short-term mTOR inhibition improved vaccine response in older adults.
This was important because rapamycin is often thought of as an immunosuppressing drug. The study suggested that dose and schedule matter. Low-dose or intermittent mTOR inhibition may improve some aspects of immune function in older people.
This is a positive study because the outcome is well defined: antibody titers. And it has clear implications. If our goal is to improve the immune response to a vaccine in older adults, rapamycin works. We need to stop and not extrapolate beyond what the study showed.
Mannick 2018: Infections
A later Mannick study, published in 2018, extended this idea, but the design was more complicated.
This was a Phase 2a randomized, placebo-controlled trial in 264 older adults. Participants received low-dose mTOR-inhibitor therapy for 6 weeks.
This study did not test rapamycin itself. It tested rapamycin-pathway drugs, including everolimus and dactolisib, alone or in combination.
The strongest signal came from a low-dose combination treatment. This group had fewer reported infections over the following year. The study also found increased activity of antiviral gene programs and improved flu-vaccine response.
Together, the 2014 and 2018 studies suggest that mTOR-pathway drugs can affect immune aging in humans in relation to an immune response to a vaccine and infections. That is the strongest positive human signal so far.
Topical Rapamycin in Skin
Another human study tested topical rapamycin for skin aging.
In this small randomized study, adults over 40 applied rapamycin to one hand and a placebo to the other. The study reported reductions in p16INK4A, a marker linked to cellular senescence, and increases in collagen VII, a protein important for skin structure.
This suggests rapamycin can affect aging-related markers in human tissue. But it was a local skin study, not a systemic aging or brain-aging study. Another example where rapamycin wins in well-defined outcomes with clear readouts.
Rapamycin and Exercise
However, a small exercise study raises an important caution. One effect on skin or a vaccine response does not mean better health.
In this 13-week randomized trial, 40 sedentary older adults received either once-weekly low-dose rapamycin or a placebo while doing a light home exercise program.
The expectation was that rapamycin might improve exercise benefits by improving aging biology. The signal went the other way.
The placebo group improved more than the rapamycin group on some physical-function measures. The clearest difference was in the 30-second sit-to-stand test, a simple measure of lower-body strength and function. Grip strength and self-rated well-being also reportedly favored the placebo. Side effects such as soreness and fatigue were more common in the rapamycin group, and one serious infection was reported.
This study was small and short. It does not prove that rapamycin always blunts exercise benefits. But it matters because exercise is one of the strongest proven interventions for healthy aging and dementia prevention.
Exercise works by creating a controlled stress. Muscle is challenged, then rebuilds stronger. That rebuilding requires mTOR. If rapamycin is active during the recovery window, it may interfere with the muscle’s ability to adapt. We saw something similar with metformin, albeit via a different mechanism.
So, To Rapamycin or Not To Rapamycin? Paraphrasing Shakespeare
In humans, the clearest positive signals are the immune response and selected tissue markers. Rapamycin-like drugs have improved vaccine response in older adults. A later study suggested fewer infections in selected treatment groups. Topical rapamycin changed some aging-related markers in skin.
These are real biological signals.
But they are not the same as showing that rapamycin slows human aging, protects the brain, or prevents Alzheimer’s disease.
That distinction is the main point.
For Alzheimer’s prevention, we would want evidence that rapamycin improves meaningful brain-related outcomes: amyloid, tau, neurodegeneration, brain inflammation, cognition, or dementia risk.
We do not have that evidence.
Instead, the field has mostly shown that rapamycin can change selected immune or tissue readouts under specific conditions. That is interesting biology. It is not yet a prevention therapy.
Where the Field Seems to Be Moving
The most active human work no longer seems to be “rapamycin for everyone to slow aging.”
It seems to be moving toward more specific questions:
Can rapamycin improve immune aging?
Can it slow ovarian aging?
Can it affect periodontal disease?
Can it change skin aging markers?
Can it be timed or dosed in a way that preserves benefit while avoiding harm?
That shift is important. It suggests that the field recognizes the main problem: aging is not one pathway, and rapamycin is not one simple anti-aging switch.
A useful rapamycin trial needs a clear biological target and a clear readout.
For Alzheimer’s prevention, we do not have that.
The Real Missing Piece: Immune-Aging Biomarkers
The biggest lesson from rapamycin is not only about rapamycin.
It is about measurement.
For cardiovascular disease, we can measure blood pressure, ApoB, LDL cholesterol, HbA1C, and other risk factors. We can treat those risk factors and track whether the treatment worked.
For immune aging, we do not have an equivalent.
We can measure antibody response after a vaccine. That is useful, but it is only one test of one part of the immune system. It does not tell us whether rapamycin improved brain aging, neuronal autophagy, senescent-cell burden, or Alzheimer’s risk.
This is the central challenge.
To use rapamycin intelligently, we would need biomarkers that tell us who has the kind of aging biology rapamycin can improve, what dose is enough, whether the drug hit the intended pathway, and whether the benefit is worth the risk.
That is hard because the human immune system is not one number. It is shaped by age, sex, infections, vaccines, metabolism, obesity, sleep, exercise, medications, genetics, chronic inflammation, and decades of immune memory.
So the future of rapamycin may depend less on enthusiasm and more on biomarkers.
Not “Who wants to try rapamycin?”
But: Who has the biology that rapamycin is likely to improve, and how will we know it worked? And in what organ? Topical for skin aging? Adjuvant to a vaccine?
Rapamycin and Alzheimer’s Prevention
Rapamycin has a plausible connection to Alzheimer’s biology. mTOR is linked to autophagy, metabolism, inflammation, immune aging, and synaptic function. These all matter for brain aging.
But plausibility is not proof.
For someone with a genetic risk for Alzheimer’s disease, the key question is not whether rapamycin is biologically interesting. It is. The question is whether the existing human studies show a prevention effect.
They do not.
Today, I would not recommend rapamycin for Alzheimer’s prevention outside a clinical trial.
The Risk Side
Rapamycin is not a supplement. It is a real drug.
It can affect immunity, cholesterol and triglycerides, blood sugar, wound healing, mouth ulcers, infection risk, and drug interactions. The risk depends on dose, schedule, age, baseline health, and other medications.
Some people argue that once-weekly low-dose rapamycin may avoid many problems seen with daily immune-suppressing doses.
That may be true.
But “may be safer” is not the same as “proven safe for long-term prevention in healthy people.”
Prevention raises the bar. A prevention drug must be very safe, because many people taking it may never develop the disease they are trying to avoid.
Areas of Uncertainty
Several questions remain unanswered.
What is the right dose?
Is weekly dosing better than daily dosing?
Should rapamycin be used only in older adults?
Does APOE genotype matter?
Does baseline inflammation matter?
Does metabolic health matter?
Does rapamycin help people who already exercise, sleep well, and have good metabolic health?
Could it blunt exercise adaptation in some settings?
Can it improve Alzheimer’s biomarkers?
Most importantly: what specific outcome? That determines whether it is working.
Until we can answer these questions, use for aging or Alzheimer’s prevention is not recommended.
What I Would Tell My Friend
I would tell my friend that rapamycin is scientifically important, but not ready for Alzheimer’s prevention.
For now, I would focus on interventions with stronger human evidence: exercise, blood pressure control, sleep, metabolic health, hearing, social connection, vascular risk reduction, and treatment of insulin resistance or diabetes when present.
The next step is better and targeted trials with better immune-aging biomarkers tied to outcomes more concrete than human aging.
Take-Home Messages
Rapamycin is one of the most compelling anti-aging drugs in mouse studies.
Mouse lifespan extension does not prove human benefit.
Alzheimer’s mouse-model data are useful for understanding mechanisms, but they do not prove Alzheimer’s prevention in humans.
Human trials exist, but the strongest positive evidence is improved vaccine response and fewer infections in selected settings.
Low-dose rapamycin may improve immune response by reducing age-related immune dysfunction, not by simply “boosting” the immune system.
Rapamycin may interfere with exercise adaptation if mTOR is suppressed during the muscle-rebuilding window.
The human studies so far do not show that rapamycin works in people the way it works in mice.
We do not yet have convincing evidence that rapamycin improves Alzheimer’s biomarkers such as amyloid, tau, neurodegeneration, or cognition.
The biggest missing piece is a practical immune-aging biomarker that tells us who might benefit and whether the drug worked.
Rapamycin is a real drug with real risks, especially if used long-term.
For aging or Alzheimer’s prevention, the current evidence does not justify rapamycin use today.
The right conclusion is not “rapamycin does not work.” The better conclusion is: what is a better indication for rapamycin? And how do we design smarter trials?
Key References
Harrison DE, Strong R, Sharp ZD, et al. Rapamycin fed late in life extends lifespan in genetically heterogeneous mice. Nature. 2009.
Miller RA, Harrison DE, Astle CM, et al. Rapamycin-mediated lifespan increase in mice is dose and sex dependent and metabolically distinct from dietary restriction. Aging Cell. 2014.
Caccamo A, Majumder S, Richardson A, Strong R, Oddo S. Molecular interplay between mTOR, amyloid-beta, and tau: effects on cognitive impairments. Journal of Biological Chemistry. 2010.
Mannick JB, Del Giudice G, Lattanzi M, et al. mTOR inhibition improves immune function in the elderly. Science Translational Medicine. 2014.
Mannick JB, Morris M, Hockey HP, et al. TORC1 inhibition enhances immune function and reduces infections in the elderly. Science Translational Medicine. 2018.
Chung CL, Lawrence I, Hoffman M, et al. Topical rapamycin reduces markers of senescence and aging in human skin: an exploratory, prospective, randomized trial. GeroScience. 2019.
Kaeberlein M, Galvan V. Rapamycin and Alzheimer’s disease: time for a clinical trial? Science Translational Medicine. 2019.
I enjoyed this piece as it highlights one of the most important lessons in translational aging research: remarkable results in mice do not automatically translate into humans. Rapamycin remains one of the most intriguing longevity interventions, but the gap between extending lifespan in animal models and improving human healthspan is where the real challenge lies. As a physician-scientist, I believe it’s important for both doctors and patients to distinguish enthusiasm from evidence. The mechanistic rationale for mTOR inhibition is compelling, and preclinical data are impressive, but questions regarding dosing, timing, safety, and long-term outcomes in humans remain largely unanswered. Biology is rarely as straightforward as it appears in model organisms. Perhaps the “rapamycin problem” is really a reminder that longevity medicine requires both curiosity and humility. Translating promising science into meaningful human benefit is far more complex than reproducing results in mice. Thanks for sharing this thoughtful and nuanced perspective!
Appreciate the balanced review, Dr. Yassine. I agree that we don't yet have human evidence showing rapamycin prevents Alzheimer's disease.
That said, some of us with APOE4/4 don't have the luxury of waiting decades for perfect data. We make decisions based on the totality of evidence available today: mechanistic data, animal studies, observational experience, individual risk profiles, and personal risk tolerance.
The late Dr. Alan Green (I was his patient from 2021 until he passed in September 2024) believed one of rapamycin's most important potential benefits for APOE4 carriers was protection of the blood-brain barrier. The APOE4-associated CypA–NFκB–MMP9 pathway leading to pericyte injury and BBB dysfunction remains, in my view, a compelling biological rationale for intervention, even if it has not yet been proven in humans.
For me, the question isn't whether rapamycin is proven. It isn't. The question is whether the potential benefit outweighs the potential risk in someone already carrying a substantially elevated lifetime risk of Alzheimer's disease. My answer remains yes.
My personal experience with once-weekly 6 mg rapamycin over the past several years has been uneventful. I take periodic breaks to allow washout and skip doses around dental procedures or other situations where infection risk may be increased. Dr. Green also encouraged practical precautions and ensured his patients had a Z-Pak on hand for prompt treatment should an infection arise.
For now, based on the available science, I will definitely continue taking rapamycin.