

While You Were Sleeping
How Your Brain Cleans Itself -- and What It Means for Alzheimer's

Happy Memorial Day to all of you. Memorial Day is a time to remember lives lost in service and to reflect seriously on the human cost of war.
It is also a good moment to think about rest, recovery, and the quiet biological work the brain does when the day finally ends.
Consider a 56-year-old man -- let’s call him David.
David works in the media industry, where deadlines, breaking news, public pressure, and long screen-heavy days can make work unusually stressful.
He recently learned that he carries two copies of APOE4, the strongest common genetic risk factor for late-onset Alzheimer’s disease.
He occasionally loses a word mid-sentence.
He eats well, exercises daily, and keeps a healthy weight.
But one pattern stands out: he wakes around 4 a.m., lies there exhausted, and cannot fall back asleep.
Most evenings, he watches television late.
He feels anxious at night.
A few times a week, he has caffeine in the afternoon or wine with dinner.
This post is written for him -- and for anyone wondering whether sleep is just rest, or something more active and protective.
I am grateful to my colleague and friend Dr. Miranda Lim -- neuroscientist, sleep researcher, and expert in sleep and neurodegeneration -- for her generous feedback on this piece.
1. The Brain’s Nightly Cleaning Crew
Sleep is active brain maintenance.
It is not simply the absence of being awake.
During sleep, fluid moves through the spaces around brain cells and helps wash away metabolic waste.
This system is called the glymphatic system -- glial because it depends on support cells in the brain, and lymphatic because it behaves like a drainage system.
Among the waste products it helps clear are amyloid-beta and tau, two proteins central to Alzheimer’s disease.
In a landmark mouse study, the brain cleared waste far more efficiently during sleep than during wakefulness [1].
Other studies have shown that amyloid and tau follow sleep-wake rhythms, rising during wakefulness and falling during sleep [2,3].
One bad night does not cause Alzheimer’s.
But repeated sleep disruption, year after year, may remove one layer of protection from a brain that is already aging.
The relationship runs in both directions.
Poor sleep may worsen amyloid and tau biology.
Early amyloid and tau changes may also damage the brain circuits that regulate sleep, making sleep more fragmented over time [4].
2. APOE4 and Sleep: Why David’s Night Matters
Why might sleep matter more in APOE4 carriers?
One way to think about it is this: APOE4 may make amyloid handling less efficient and the brain’s immune response more reactive.
If the nightly clean-up system is also weakened by insomnia, sleep apnea, alcohol, irregular timing, or anxiety, the same amount of sleep disruption may carry a higher cost.
Human studies suggest that sleep and APOE4 interact.
In older adults, better sleep consolidation appeared to weaken the relationship between APOE4 and Alzheimer ’s-related pathology [5].
Newer work also suggests that sleep disturbance may be more strongly linked to amyloid burden in APOE4 carriers than in non-carriers [6].
Animal work supports the same idea: APOE4 and sleep disruption can act together to accelerate amyloid and tau-related changes [7].
The practical point is leverage.
David cannot change his genes.
But he can change the nightly environment his genes operate in.
For an APOE4 carrier, treating insomnia, sleep apnea, irregular sleep timing, alcohol-related sleep fragmentation, and nighttime anxiety is not cosmetic wellness.
It is risk management.
3. Not All Sleep Is Equal: Understanding the Cycles
Adults usually need seven to nine hours of sleep.
But quality matters as much as quantity.
Sleep moves through stages in cycles of roughly 90 to 120 minutes.
Most people cycle through these stages three to five times per night.
A typical night is not flat.
It looks like a staircase: deeper sleep early in the night, then longer stretches of dream-rich REM sleep toward morning.
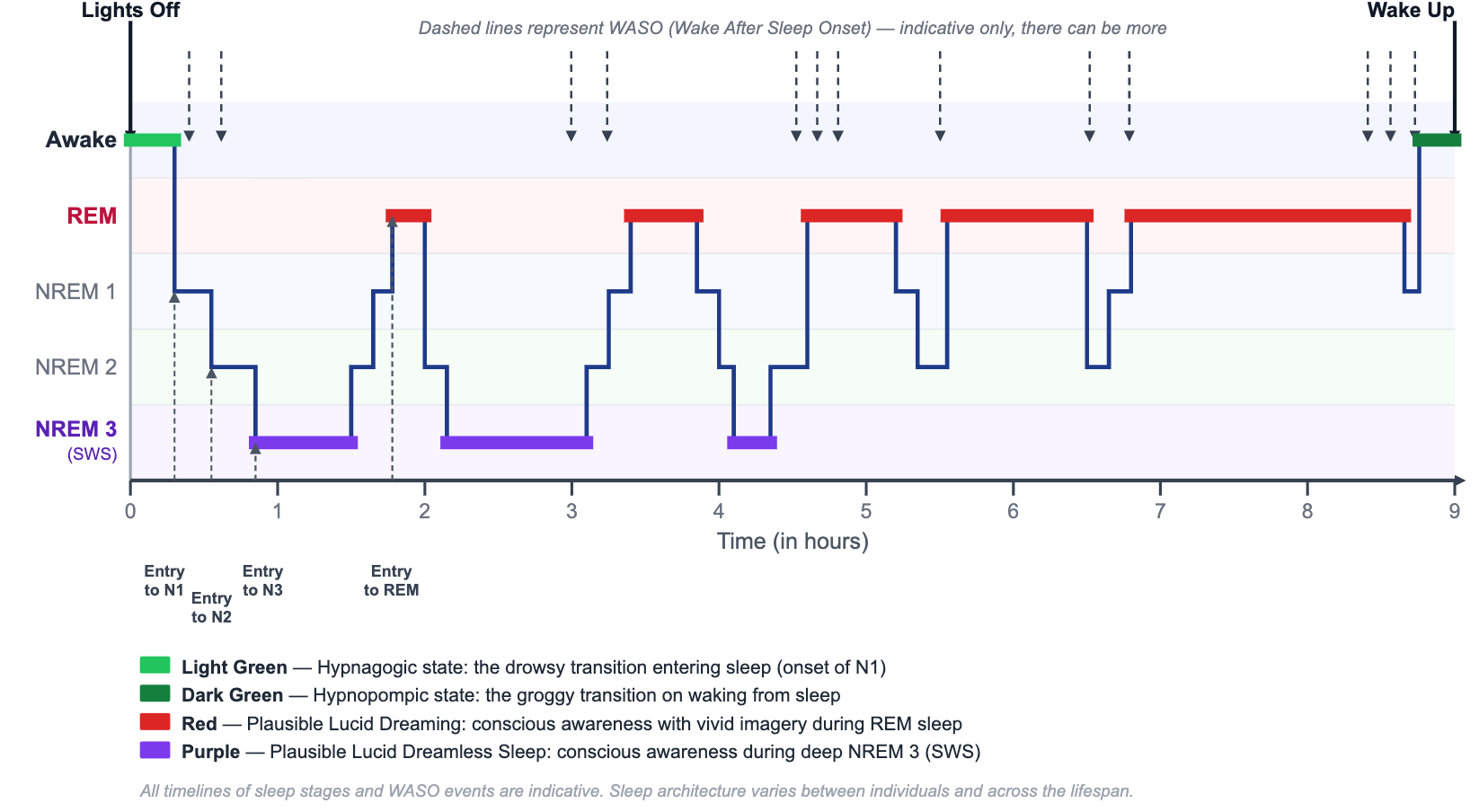
Figure: Sleep cycles across a typical night. Deep sleep is more common early in the night. REM sleep lengthens toward morning. Adapted from Shah et al., Portable Monitoring, 2013.
The light green zone at the beginning is the hypnagogic state. This is the drifting period when thoughts loosen, images appear, and the brain crosses from wakefulness into sleep. Its mirror image is the hypnopompic state, the groggy transition that happens while waking. Both are normal borderlands between consciousness and sleep.
NREM Stage 1, or N1, is the lightest stage of sleep — the brief doorway between wakefulness and sleep, when thoughts loosen, awareness fades, and the hypnagogic state begins.
NREM Stage 2 is the workhorse of the night. It often makes up about half of total sleep and is marked by sleep spindles, brief bursts of brain activity involved in memory processing.
NREM Stage 3 is deep sleep, also called slow-wave sleep (SWS). This stage is linked to physical restoration, immune signaling, memory stabilization, and possibly glymphatic clearance. The purple segments in the figure refer to lucid dreamless sleep. This is a rare state, reported especially among experienced meditators, in which a person may have clear awareness during deep sleep without the usual story, images, or dream content.
Deep sleep declines with age. A long-term study in JAMA Neurology found that lower slow-wave sleep was associated with higher dementia risk, although the study was observational and cannot prove cause and effect [8].
REM sleep is the stage of vivid dreams. The brain is highly active, but the body is temporarily paralyzed, so we do not act out dreams. Some people experience lucid dreaming during REM: they realize they are dreaming while the dream is still happening, and sometimes can influence the dream. REM helps process emotion, fear, anxiety, and complex memories. Alcohol, sleep apnea, and some medications can fragment or suppress REM.
The dashed arrows mark brief returns toward wakefulness, often called WASO -- wake after sleep onset. Tiny awakenings happen to everyone. The problem is not waking for a moment. The problem is waking and staying awake for 20 minutes or more.
The goal is not to force one stage at the expense of another. The brain needs the full natural sequence: light sleep, Stage 2, deep sleep, REM, and brief awakenings that quickly return to sleep.
David’s 4 a.m. awakening may begin as a normal sleep-cycle boundary. It also occurs in the part of the night when REM sleep is usually longer and more frequent. If anxiety fragments this REM-rich period, the night may feel as if it ends too early.
4. Start With a Sleep Audit
Before buying devices or supplements, start with a simple sleep diary.
Track for at least two to three weeks, including weekends.
Each morning, write down bedtime, wake time, estimated total sleep, number of awakenings, and how refreshed you feel.
If you wake during the night, estimate how long it takes to fall back asleep.
Each evening, note caffeine timing, alcohol, exercise, screen exposure, and anxiety level.
Anxiety deserves its own line in the diary.
It is one of the most common and underrecognized sleep disruptors.
For David, the diary might reveal a pattern: caffeine after 2 p.m., television until 11 p.m., wine with dinner, and then a 4 a.m. awakening.
None of these is dramatic alone.
Together, they can fragment sleep.
The goal is not perfection.
The goal is pattern recognition.
5. Six Habits With the Best Evidence
Keep a steady schedule.
Wake up at the same time every day, including weekends.
A stable wake time is one of the strongest signals to the body clock.
Protect the last hour.
Dim lights after dinner.
Avoid emotionally charged television, work email, and bright screens close to bed.
Blue-wavelength light suppresses melatonin, the hormone that tells the brain darkness has arrived.
Keep the bedroom cool.
A room around 65 to 68 degrees F, or 18 to 20 degrees C, helps the body drop its core temperature, which supports sleep onset and deep sleep.
Cut caffeine early.
Caffeine can last five to seven hours, and often longer in older adults.
What was harmless at 35 may be disruptive at 56.
Do not use alcohol as a sleep aid.
Alcohol may help you fall asleep faster, but it fragments the second half of the night and suppresses deep sleep and REM.
Move your body daily.
Regular exercise improves sleep pressure, mood, insulin sensitivity, and cardiovascular health.
Avoid vigorous exercise close to bedtime if it leaves you wired.
6. Treat Anxiety and Insomnia Together: Why CBT-I Matters
Many people think insomnia is a nighttime problem.
Often, it is also a daytime anxiety loop.
The brain starts to learn that the bed is a place for effort, monitoring, frustration, and worry.
That learned association is called conditioned arousal.
CBT-I -- Cognitive Behavioral Therapy for Insomnia -- is designed to break that loop.
It is not simply sleep hygiene.
CBT-I combines stimulus control, sleep scheduling, cognitive therapy, relaxation skills, and careful adjustment of time in bed.
It helps the brain relearn a simple rule: bed equals sleep, not struggle.
The American College of Physicians recommends CBT-I as the initial treatment for chronic insomnia in adults [9].
AASM guidance also supports behavioral-psychological treatment and, when medication is needed, pairing it with CBT-I rather than using medication alone [10].
For David, CBT-I is especially relevant because anxiety may be shortening or fragmenting the REM-rich final third of his night.
The goal is not to convince him to stop worrying by willpower.
The goal is to change the sleep system so his body no longer practices worry at 4 a.m.
CBT-I can be done with a trained therapist, through some sleep clinics, or through validated digital CBT-I programs when access is limited.
It can feel uncomfortable at first because it asks people to change habits that feel protective.
But unlike sedatives, it teaches a durable skill.
7. When to Refer to a Sleep Specialist
Not every sleep problem needs a sleep lab.
But some do.
Refer for evaluation if there is loud snoring, witnessed pauses in breathing, gasping, choking, morning headaches, dry mouth, high blood pressure, or daytime sleepiness despite enough time in bed.
These are red flags for obstructive sleep apnea.
Sleep apnea repeatedly drops oxygen and forces the brain to wake just enough to breathe.
That can destroy deep sleep and REM without the person remembering the awakenings.
Referral is also appropriate when insomnia lasts more than three months, causes daytime impairment, or does not improve with basic behavioral steps.
Other reasons include restless legs, violent dream enactment, narcolepsy symptoms, shift-work disorder, complex medication questions, or persistent early-morning awakening with depression or severe anxiety.
For older adults and APOE4 carriers, the threshold can be lower.
A treatable sleep disorder is not something to watch passively.
8. Sleep Medications: Useful, but Not the Same as Natural Sleep
There are times when sleep medication is reasonable.
Jet lag, a hospital stay, acute grief, or a short period of severe insomnia may justify short-term help.
The problem is assuming that a pill that causes unconsciousness is the same as healthy sleep.
Many common sleep aids -- benzodiazepines, Z-drugs such as zolpidem, and over-the-counter antihistamines such as diphenhydramine -- sedate the brain.
They may reduce the memory of waking up.
But they can also alter sleep architecture, suppress REM or deep sleep, increase falls, and create dependence or rebound insomnia.
This matters even more in older adults.
Antihistamine sleep aids have anticholinergic effects, which are generally a poor fit for brain health when used chronically.
Newer orexin receptor antagonists, such as suvorexant and lemborexant, work differently.
They reduce the brain’s wakefulness signal rather than broadly sedating the brain.
They may preserve sleep architecture more faithfully, but they still require medical supervision and their long-term effects are still uncertain.
Melatonin belongs in a separate category.
It is not a sedative.
It is a darkness signal that can help shift the body clock for jet lag or delayed sleep timing.
Low doses, often 0.5 to 1 mg, are usually enough for circadian purposes.
More is not necessarily better.
Do not take melatonin before driving.
9. Rings, Watches, and New Sleep Technologies
Sleep devices can be helpful when they are used for trends, not truth.
A ring or watch can show bedtime regularity, total sleep opportunity, heart rate patterns, movement, and whether weekends are drifting later.
For David, a device might show that his sleep is shorter after wine or caffeine, or that his weekend schedule shifts by two hours.
But consumer devices are not sleep labs.
They usually estimate sleep from movement, heart rate, temperature, and algorithms.
They do not directly measure brain waves the way polysomnography does.
Recent validation studies suggest many devices are fairly good at estimating sleep versus wake, but less reliable at distinguishing deep sleep from REM or light sleep [11].
This is why a low deep sleep score should not create panic.
And a beautiful sleep score should not override symptoms like snoring, gasping, or daytime sleepiness.
The best use is pattern recognition.
Use the device to ask: what happens when I keep a steady wake time, stop alcohol, treat anxiety, or get morning light?
The worst use is sleep perfectionism.
Some people become more anxious because they chase a score, a problem sometimes called orthosomnia.
If tracking makes sleep feel like a test, stop tracking for a while and return to a diary.
On the research frontier, more advanced tools are emerging.
Wearable EEG headbands can measure brain activity more directly and may eventually guide gentle stimulation during naturally occurring deep sleep transitions [12].
Other experimental tools are trying to measure glymphatic function in humans during sleep [13,14].
They are not yet a substitute for the basics: regular timing, darkness at night, morning light, exercise, apnea treatment, and anxiety care.
10. What We Still Do Not Know
Sleep and Alzheimer’s influence each other in both directions.
Poor sleep may increase amyloid and tau.
But early Alzheimer’s changes can also damage the brain circuits that regulate sleep.
That makes cause and effect hard to untangle.
We do not yet know the exact amount of deep sleep needed for brain clearance.
We do not know whether every APOE4 carrier benefits equally from sleep intervention.
We do not know whether fixing sleep after symptoms begin can slow disease progression.
So the honest answer is this: sleep is not a cure for Alzheimer’s.
But it is one of the most biologically plausible, low-cost, and broadly beneficial targets we have.
Take-Home Messages
· Sleep is active brain maintenance. The glymphatic system helps clear amyloid-beta, tau, and other waste during sleep.
· APOE4 raises the stakes, not destiny. Genes are not fate, but APOE4 may make good sleep more important.
· All sleep stages matter. Deep sleep may support clearance, REM supports emotional and memory processing, and the full cycle matters more than any single stage.
· Brief awakenings are normal. Lying awake for 20 minutes or more is the pattern to address.
· Treat anxiety as part of treating sleep. CBT-I directly targets the 4 a.m. worry loop.
· Refer when red flags appear. Snoring, gasping, witnessed pauses, daytime sleepiness, restless legs, unusual nighttime behaviors, or chronic insomnia deserve evaluation.
· Use devices wisely. Rings and watches can reveal patterns, but they are not diagnostic tests and should not become another source of anxiety.
· Be careful with sedatives. Unconsciousness is not the same as natural sleep.
For David, the prescription is not fear.
It is a plan: protect the night, treat the disruptors, and give the brain the conditions it needs to do its quiet work.
References
1. Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373-377.
2. Kang JE, Lim MM, Bateman RJ, et al. Amyloid-beta dynamics are regulated by orexin and the sleep-wake cycle. Science. 2009;326(5955):1005-1007.
3. Holth JK, Fritschi SK, Wang C, et al. The sleep-wake cycle regulates brain interstitial fluid tau in mice and CSF tau in humans. Science. 2019;363(6429):880-884.
4. Vanderheyden WM, Lim MM, Musiek ES, Gerstner JR. Alzheimer’s disease and sleep-wake disturbances: amyloid, astrocytes, and animal models. Journal of Neuroscience. 2018;38(12):2901-2910.
5. Lim ASP, Yu L, Kowgier M, Schneider JA, Buchman AS, Bennett DA. Sleep modifies the relation of APOE to risk of Alzheimer disease and neurofibrillary tangle pathology. JAMA Neurology. 2013;70(12):1544-1551.
6. Liang Q, et al. Moderating effect of APOE epsilon4 on the association of sleep disturbance with regional amyloid-beta burden in cognitively normal older adults. Frontiers in Aging Neuroscience. 2025.
7. Wang C, Nambiar A, Strickland MR, et al. APOE-epsilon4 synergizes with sleep disruption to accelerate amyloid-beta deposition and plaque-associated tau seeding and spreading. Journal of Clinical Investigation. 2025.
8. Himali JJ, Baril A-A, Cavuoto MG, et al. Association between slow-wave sleep loss and incident dementia. JAMA Neurology. 2023;80(11):1326-1333.
9. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Annals of Internal Medicine. 2016;165(2):125-133.
10. Buysse DJ, et al. Combination treatment for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. Journal of Clinical Sleep Medicine. 2026.
11. Robbins R, Weaver MD, Sullivan JP, et al. Accuracy of three commercial wearable devices for sleep tracking in healthy adults. Sensors. 2024;24(20):6532.
12. Hathaway E, Morgan K, Carson M, et al. Transcranial electrical stimulation targeting limbic cortex increases the duration of human deep sleep. Sleep Medicine. 2021;81:350-357.
13. Dagum P, Giovangrandi L, Levendovszky SR, et al. A wireless device for continuous measurement of brain parenchymal resistance tracks glymphatic function in humans. Nature Biomedical Engineering. 2025;9:1656-1676.
14. Dagum P, Elbert DL, Giovangrandi L, et al. The glymphatic system clears amyloid beta and tau from brain to plasma in humans. Nature Communications. 2026;17(1):715.
When I learned of my APOE4 status the first thing I did was improve sleep hygiene. I spent most of my working life thinking 4 hours of sleep and being the first one into work and the last to leave would elevate my career. It didn't. Being a workaholic takes a serious toll on your body systems. I now get 7-8 hours of quality sleep per night. I highly recommend separate bedrooms with separate temperature controls for couples. Hubby prefers to sleep in nursing home temps. My room is 67-68°. I wake as a happier, kinder person after a good night's sleep.
Another excellent article Dr. Yassine. thank you.