

Taurine, ALZ-801, and the Long Road to an Alzheimer’s Drug
Why Alzheimer’s science demands both hope and caution

A husband and wife came to see me in clinic.
She was 63 years old. She had two copies of APOE4, the strongest common genetic risk factor for late-onset Alzheimer’s disease. Over the previous three years, her function had declined significantly. She had been diagnosed with Alzheimer’s dementia.
Her husband had seen information about ALZ-801, an investigational oral Alzheimer’s drug being developed for people with two copies of APOE4. The message was powerful: his wife had the risk gene copy, she had Alzheimer’s, and this drug seemed designed for someone like her.
He asked me a direct question: How can we get this drug to her as soon as possible?
That question is why I am writing this.
Alzheimer’s disease creates urgency. APOE4 creates a sense of precision. How can we help her?
This post is about two related stories: taurine, a naturally occurring molecule now being studied for ApoE4 biology, and ALZ-801, an investigational oral drug built around homotaurine/tramiprosate chemistry.
Both are scientifically interesting. Neither should be treated as proven.
Why ApoE4 matters
ApoE is a protein involved in fat transport and brain health. Most people carry one of three common forms: ApoE2, ApoE3, or ApoE4. ApoE4 is a major AD risk factor
One idea is that ApoE4 may be more likely than ApoE3 to misfold or clump together. That is where taurine enters the story.
A recent paper reported that taurine can reduce ApoE4 aggregation in laboratory systems, change ApoE4 protein behavior, and shift some gene patterns in ApoE4 brain organoids toward patterns seen with ApoE3.
That is interesting. But it does not mean taurine treats Alzheimer’s disease.
Why a promising lab result is not the same as a treatment
A lab result can be exciting because it gives scientists a lead. It says: this pathway might matter. But a lead is not a medicine.
To become a medicine, a molecule has to answer many questions.
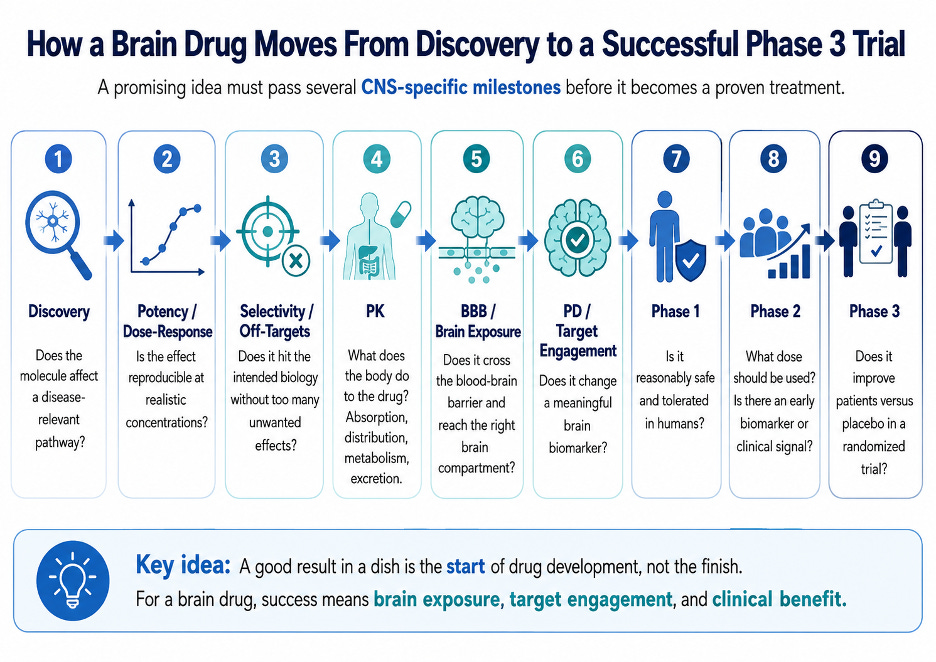
Does it work in a clear dose-response pattern? Scientists ask whether more drug produces more effect, and whether the concentration needed is realistic. For many drugs, this is measured with an IC50, the amount needed to block a process by 50 percent.
But protein clumping is messy biology. It depends on time, temperature, protein concentration, salt, assay conditions, and whether the molecule binds one specific target or weakly touches many surfaces.
That matters for taurine. In the ApoE4 paper, taurine appears to interact weakly and in multiple places. That can still matter biologically, but it is not the same as a strong, clean, highly selective drug effect.
Does it reach the brain? A molecule can work in a test tube and fail in the body. The brain is protected by the blood-brain barrier, which limits what gets from the blood into brain tissue. For an Alzheimer’s drug, reaching the brain is essential.
Does the lab dose match what people get from food or supplements? This is where translation often breaks down. In the taurine paper, the aggregation assay used 20 millimolar taurine to suppress ApoE4 aggregation, and 30 millimolar taurine to test whether pre-formed aggregates could be reduced. Those are test-tube concentrations, not dietary exposures.
A 20 millimolar taurine solution contains about 2,500 milligrams of taurine per liter. One liter of a 20 millimolar taurine solution contains roughly the taurine found in about 3.7 to 31 kilograms of beef; a 30 millimolar solution corresponds to about 5.5 to 47 kilograms. This is an imperfect comparison because a test tube is not a human body, but that is the point: eating steak does not recreate a millimolar concentration to break the apoE aggregation shown in the test tube. At least after a beefy meal!
The point is not that dietary taurine is irrelevant. The point is that foods and supplements must not be treated as if they automatically reproduce the concentrations, timing, and exposure used in laboratory experiments.
Does it have off-target effects? A molecule that weakly interacts with many surfaces may affect many pathways. Sometimes that is useful. Sometimes it creates unwanted effects. Either way, it has to be measured.
PK means pharmacokinetics: what the body does to the drug. Is it absorbed? How long does it last? Does it enter the brain? How is it cleared?
PD means pharmacodynamics: what the drug does to the body. Does it hit the intended biology? Does it move a meaningful biomarker? Does that translate into better memory or function?
A molecule can look promising and still fail because the PK is poor, the PD is weak, or the effect does not matter clinically.
This does not make the biology unimportant. It means the biology must be tested carefully before it becomes a claim about treatment.
ALZ-801: applying the drug-development ladder
ALZ-801 is different from taurine because it is not simply a supplement story. It is a drug-development story.
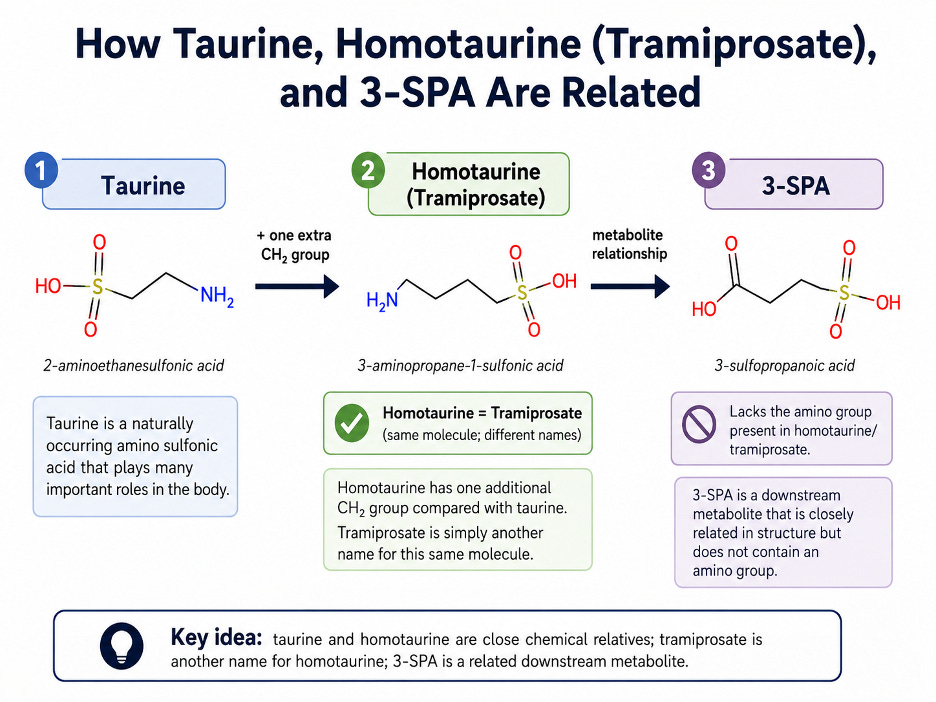
ALZ-801, also called valiltramiprosate, is a prodrug of tramiprosate. Tramiprosate is also known as homotaurine or 3-APS. Homotaurine is chemically related to taurine, but ALZ-801 is not taurine. It was designed to deliver tramiprosate more predictably in the body.
Tramiprosate was originally developed as an Alzheimer’s drug called Alzhemed. The idea was to interfere with amyloid-beta oligomers, small soluble amyloid clusters that may damage synapses before large plaques form.
The broad tramiprosate Phase 3 program did not show convincing benefit in the overall Alzheimer’s population. Later, homotaurine was sold over the counter in Canada as a memory supplement called Vivimind.
So how did this older molecule return as ALZ-801? The public story has four pieces: lab studies suggesting anti-amyloid aggregation activity; subgroup analyses suggesting a possible APOE4/4 signal; a prodrug designed for better absorption and tolerability; and a Phase 3 trial in people with early Alzheimer’s disease and two copies of APOE4.
That is a reasonable path to a Phase 3 trial. It is not a reason to assume the drug works before the randomized trial answers the question.
What ALZ-801 still had to prove
Is there a clean IC50? Not in the simple way people may imagine. ALZ-801 is not like a classic drug that blocks one enzyme at one active site. Its proposed effect is to reduce amyloid oligomer formation, which is a complex clumping process. The public development story is built around aggregation assays, stoichiometry, PK modeling, and projected brain exposure, not a single easy-to-interpret human IC50.
How was the dose chosen? Public papers describe a PK bridging strategy. The Phase 3 dose, 265 mg twice daily, was selected to produce tramiprosate exposure similar to 150 mg twice daily tramiprosate, the dose later emphasized from older APOE4/4 subgroup analyses. In other words, the dose was not chosen from a clean prospective human brain target-engagement trial; it was bridged from the older tramiprosate program and from projected exposure needed to inhibit amyloid oligomer formation.
Does it cross the blood-brain barrier? The public evidence is supportive but still indirect. The development literature describes tramiprosate and 3-SPA as brain-penetrant and refers to CSF/metabolite data, animal brain-penetration work, and projected human brain exposure. I did not find a public FDA review package that independently lays out a definitive human BBB and target-engagement analysis for ALZ-801.
What about off-target effects? ALZ-801 is usually discussed as an amyloid-oligomer drug, but homotaurine-like molecules may have other biological effects, including possible effects on GABA receptors. That does not mean the drug is unsafe or ineffective. It means the mechanism should not be oversimplified.
What is the PD readout? Cognition is not the PD readout. Cognition is the clinical outcome. A cleaner PD readout would show that the drug changed Alzheimer’s biology in humans, such as a prespecified change in p-tau217, p-tau181, amyloid measures, GFAP, NfL, or another biomarker connected to disease activity. A convincing story would line up exposure, brain penetration, target engagement, biomarker movement, and clinical benefit.
The data on ALZ-801 are still incomplete.
Timing matters: preventing amyloid clumps is not the same as removing them
Amyloid biology unfolds over years. Amyloid-beta can misfold, form small oligomers, seed further aggregation, and eventually contribute to plaques. By the time someone has memory symptoms, especially someone with two copies of APOE4, amyloid plaques may already be widespread. The amyloid plaques appear decades before one has a diagnosis of mild cognitive impairment.
That matters for ALZ-801. If a drug mainly prevents new amyloid oligomers from forming, when is the best time to use it? Before plaques form? Around the time amyloid is seeding? After plaques are already present?
Does ALZ-801 dissolve existing plaques? Does it reduce amyloid PET signal? Does it prevent plaques from shedding toxic oligomers? Does it slow downstream tau spread? Or does it need to be used earlier than the stage when most patients are diagnosed?
These questions remain open. This does not mean ALZ-801 cannot work. It means the timing of treatment may be critical and that there are many unaswered questions still.
The problem with confidence before placebo-controlled evidence
The path to ALZ-801 included lab studies, improved PK, brain-penetration arguments, APOE4 subgroup signals, and open-label Phase 2 biomarker studies. That may be enough to justify a Phase 3 trial. It is not enough to assume success.
Open-label Phase 2 studies can help with safety, dosing, tolerability, and biomarker hypotheses. But they cannot prove clinical efficacy in Alzheimer’s disease. Without a placebo group, it is hard to know whether apparent cognitive stabilization reflects the drug, patient selection, natural history, missing data, expectations, or analysis choices.
The company’s 2023 press release claimed 31% reduction in plasma p-tau181 at 24 months, 28% preservation of hippocampal volume compared with matched ADNI external controls, and improvement on cognitive tests at 6 months with sustained stabilization above baseline for 24 months. It also stated that treated patients had a 24% improvement on RAVLT Total Score compared with matched ADNI subjects
But there was no placebo arm. Matching to ADNI is not the same as having a placebo arm. FDA standards for drug approval still require evidence that can distinguish a real drug effect from placebo effect, spontaneous change, or biased observation.
But it can become a loophole in the public narrative. When open-label data are described as clinical improvement or treatment benefit, readers may hear proof where the study design only supports a hypothesis. That is especially risky in Alzheimer’s disease, where patients and families are actively searching for options.
What did APOLLOE4 report?
APOLLOE4 tested valiltramiprosate in people with early Alzheimer’s disease who had two copies of APOE4. It was randomized, double-blind, and placebo-controlled. That was the right test.
The overall clinical result was negative. The trial did not meet its primary cognitive endpoint in the overall study population. That is the anchor result.
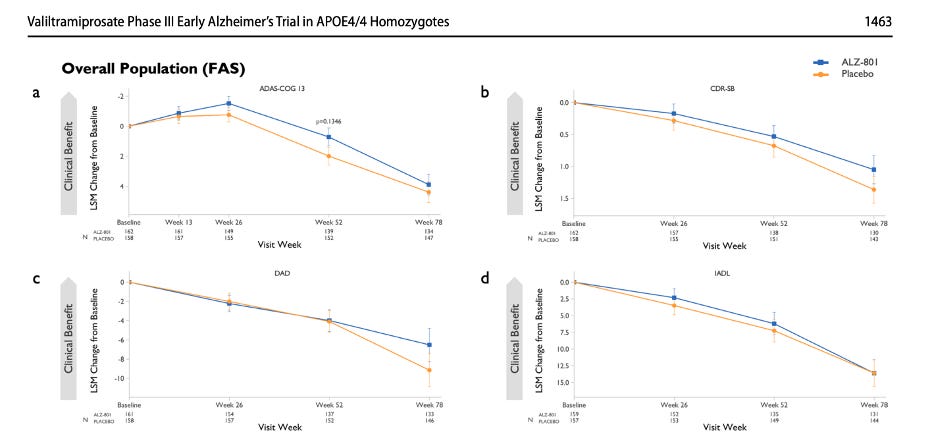
Fig: In the overall APOLLOE4 Phase 3 population, ALZ-801 did not show a statistically significant clinical benefit over placebo on the primary cognitive endpoint, ADAS-Cog13, or on key functional measures. The ALZ-801 and placebo curves separate modestly on some outcomes, but the trial did not meet its primary endpoint, so these results do not establish clinical efficacy.
The trial did report slowing of hippocampal atrophy on MRI and nominally significant clinical findings in a prespecified mild cognitive impairment subgroup. These findings are worth studying. They may justify a new trial focused on earlier-stage patients.
But they do not erase the main result: the overall Phase 3 clinical endpoint was not met. Secondary endpoints and subgroup findings can fail when tested directly in a new trial. The responsible next step is to test the MCI hypothesis prospectively, not to promote the drug publicly as if an MCI indication has already been proven.
What about biomarkers? The peer-reviewed Phase 3 paper reports that plasma biomarkers were collected, including Aβ42, Aβ40, p-tau181, p-tau217, GFAP, and NfL. But it also says that serial assessments of core Alzheimer’s plasma biomarkers were still in progress and would be reported separately.
Alzheon later announced p-tau217 results, including decreases beginning at 26 weeks, larger effects in the MCI subgroup, and correlations with cognition, function, and hippocampal volume. Those results should be taken seriously, but they are not the same as a complete, independently interpreted, peer-reviewed biomarker package with all methods, subgroup definitions, missing-data handling, and statistical corrections clearly shown.
Being conservative is not being dismissive
There is an urgent need for safe, accessible treatments for APOE4 patients. The approved anti-amyloid antibodies are difficult treatments. They require infusions, MRI monitoring, infrastructure, and careful safety discussions. APOE4 carriers, especially APOE4 homozygotes, face particular safety concerns.
An oral drug with good safety, brain penetration, and real disease-modifying benefit would be a major advance. So the goal is not to dismiss ALZ-801. The goal is to leave room for it to succeed without treating success as already proven.
If future trials in earlier APOE4/4 patients show consistent clinical benefit, supported by clear biomarker movement and acceptable safety, that would matter.
But until then, the fairest summary is this: ALZ-801 has a rational mechanism, improved PK compared with older tramiprosate, a plausible but not fully independently verified brain-exposure argument, and company-reported biomarker signals. It also missed its primary clinical endpoint in the overall APOLLOE4 Phase 3 population. The MCI signal is a reason to study the drug further, not a reason to market it to the public as proven for MCI.
What if a patient wants to take the risk?
This is the hardest question in clinic. Some APOE4 carriers and families may say: if the drug appears safe and the disease is devastating, why not try it?
That instinct is understandable. But risk is not only side effects. There is also the risk of false hope, cost, distraction from proven care, delay in planning, and loss of trust if the promise does not hold. A drug with few obvious side effects can still fail to help, and an unproven treatment can still change decisions.
The right answer is not to block hope. It is to keep hope inside a system that can tell whether the drug truly works. For now, that means carefully designed trials, transparent communication, and avoiding public claims that go beyond the evidence.
The danger of direct-to-consumer promises
The husband in my clinic was responding to a message that seemed to match his wife’s biology. That is why direct-to-consumer communication about investigational Alzheimer’s drugs must be handled carefully.
Alzheimer’s disease is devastating. APOE4 status can make a drug feel personally targeted. Families may hear developed for APOE4/4 and ask why they cannot access it now. A company may communicate through emails, websites, newsletters, webinars, advocacy groups, trial-recruitment materials, or advertisements. Some of that communication may be legal. Some of it may be framed as education.
But legal is not the same as scientifically responsible.
When a company contacts consumers with language that implies benefit before benefit has been proven, or highlights a subgroup such as MCI after the overall Phase 3 trial missed its primary endpoint, it risks turning scientific uncertainty into marketing. The audience includes patients, spouses, adult children, and caregivers making decisions under pressure.
False or overstated promises can shape decisions. Families may pursue access, interpret subgroup findings as proof, delay planning, or organize expectations around a treatment whose benefit is still uncertain.
They also damage trust. If patients are led to believe that a drug is likely to help, and then Phase 3 results disappoint, many will remember that science raised their hopes and then changed the message.
Science can survive negative trials. Negative trials are part of progress. What science cannot afford is a cycle in which early biology becomes marketing, subgroup signals become promises, and families are asked to believe before the evidence is ready.
Take-home messages
• ApoE4 biology matters, and therapies tailored to APOE4 patients are urgently needed.
• Taurine is interesting, but not proven. The taurine-ApoE4 paper is a mechanistic study, not evidence that taurine prevents or treats Alzheimer’s disease.
• Food molecules are not automatically therapies. Red meat contains taurine, wine contains resveratrol, and green tea contains EGCG, but eating or drinking these foods does not reproduce the high, controlled concentrations used in many preclinical aggregation experiments.
• ALZ-801 is a serious drug-development story, but still unproven. Its dose selection and brain-exposure argument are based on public PK and bridging data, not a clean public IC50-to-human-brain target-engagement chain.
• APOLLOE4 did not meet its primary cognitive endpoint overall. MCI subgroup and secondary findings are worth studying, but they should not be promoted to the public as a proven MCI indication without a direct confirmatory trial.
• Conservative interpretation is not dismissal. An oral, safe, effective therapy for APOE4 patients would be a major advance. The evidence should be strong enough that patients can trust the claim.
References
1. Legrand A, Cerna KA, Marques SM, et al. Taurine inhibits apolipoprotein E4 aggregation. Biomedicine & Pharmacotherapy. 2026.
2. Hey JA, et al. Clinical Pharmacokinetics and Safety of ALZ-801, a Novel Prodrug of Tramiprosate in Development for the Treatment of Alzheimer’s Disease. Clinical Pharmacokinetics. 2018.
3. Hey JA, Kocis P, Hort J, et al. Discovery and Identification of an Endogenous Metabolite of Tramiprosate and Its Prodrug ALZ-801 that Inhibits Beta Amyloid Oligomer Formation in the Human Brain. CNS Drugs. 2018.
4. Abushakra S, et al. Clinical Pharmacokinetics of Oral ALZ-801/Valiltramiprosate and its Active Agents in APOE4/4 Subjects with Early Alzheimer’s Disease. Clinical Pharmacokinetics. 2025.
5. Abushakra S, et al. Clinical Efficacy, Safety and Imaging Effects of Oral Valiltramiprosate in APOE4/4 Homozygous Individuals with Early Alzheimer’s Disease: The APOLLOE4 Phase III Randomized Controlled Trial. CNS Drugs. 2025.
6. Alzforum. Alzhemed / tramiprosate therapeutic profile.
7. Alzforum. ALZ-801 therapeutic profile.
8. FDA / eCFR. 21 CFR 314.126: Adequate and well-controlled studies.
9. FDA. Fast Track designation information and FDA Global Substance Registration System note that UNII/substance records do not imply regulatory review or approval.
10. FDA. Unproven Alzheimer’s Disease Products.
11. Cleveland Clinic Journal of Medicine. Table: Taurine content of meats, seafood, and dairy products.
12. Hey JA, et al. Effects of Oral ALZ-801/Valiltramiprosate on Plasma Biomarkers, Brain Hippocampal Volume, and Cognition: Results of 2-Year Single-Arm, Open-Label, Phase 2 Trial in APOE4 Carriers with Early Alzheimer’s Disease. Drugs. 2024.
13. Alzheon. Topline Results from Pivotal APOLLOE4 Phase 3 Trial of Oral Valiltramiprosate/ALZ-801. 2025.
I can't thank you enough for your substack. Your explanations of the science are always clear and enlightening.
Thank you for this post Dr. Yassine. I agree with your analysis completely _as a scientist_. Science is built upon incremental knowledge gain through the rigorous testing of hypotheses. That approach matches the risk/reward in science: risk is that we come to false conclusions that end up wasting time and money, and hurting trust in science generally.
_As a clinician_ (which I am not, but can appreciate), I would be uncomfortable pushing unproven treatments for all the reasons you say. There are risks associated with these (many of them not known), and may distract from a patient doing the basics (diet, exercise, sleep, etc.)
_As a human with familial history of dementia_, I don't think that my risk/reward equation is the same. I have but one life to live, and every day I am making choices that will impact that life. Not pursuing a potential therapy is a decision itself. This is not to permit a blanket "try anything that might work". You still need to assess the costs and health risks of each intervention. I don't take homotaurine, for example, because the cost of sourcing it is extreme, and I'd rather place my money elsewhere. Taurine is interesting from this lens - the data is mostly mechanistic, but it's a well studied and cheap supplement. I can see viewing this as a worthwhile risk