

Obicetrapib and the Biology of Alzheimer’s Prevention
BROADWAY showed a promising p-tau217 signal. The next test is whether a lipid drug can help the right biological population.

How do we interpret AD biomarker signals?
A recent analysis from the BROADWAY trial reported that obicetrapib slowed the rise of plasma p-tau217 over 12 months in people with cardiovascular disease [1].
That finding deserves attention.
P-tau217 is one of the strongest blood biomarkers we have for Alzheimer’s disease biology. It often rises when amyloid and tau pathology are building in the brain. So when a drug changes p-tau217 in a randomized placebo-controlled study, the field should pay attention.
But the interpretation needs to stay proportional to the study design.
BROADWAY was designed as a cardiovascular lipid trial. The Alzheimer’s biomarker analysis was pre-specified, which makes it more meaningful than a purely post-hoc analysis. But it was still an analysis within a cohort built for another primary disease question.
That distinction matters.
A pre-specified biomarker signal can point us toward an important hypothesis. It does not, by itself, prove Alzheimer’s prevention, clinical benefit, or disease modification.
The question now is whether the signal reflects a real effect on Alzheimer’s biology, whether it is strongest in the right biological subgroup, and whether it eventually translates into cognition or function.
Why Obicetrapib Is Biologically Interesting
Obicetrapib blocks cholesterol ester transfer protein (CETP), a protein that helps transfer cholesterol between lipoprotein particles in the blood.
When CETP is inhibited, the lipid system is remodeled. LDL cholesterol falls. ApoB and non-HDL cholesterol fall. Lp(a) can fall. HDL cholesterol rises, and HDL particles may become larger or more functional.
That is the established biology.
This is also why obicetrapib worked in BROADWAY for its main lipid readouts. BROADWAY enrolled people with atherosclerotic cardiovascular disease (ASCVD) and/or heterozygous familial hypercholesterolemia whose LDL cholesterol remained inadequately controlled despite lipid-lowering therapy. In that population, obicetrapib lowered LDL-C, raised HDL-C, and lowered Lp(a) [1].
The Alzheimer’s question is different.
The question is whether this peripheral lipid remodeling can also influence Alzheimer’s-related biology.
There are several plausible pathways. The effect could be vascular, through lower LDL-C, ApoB, Lp(a), and improved vascular risk biology. It could be HDL-mediated, through larger or more functional HDL particles that support cholesterol efflux, antioxidant activity, and anti-inflammatory signaling. It could also involve amyloid handling, including a possible peripheral sink effect where remodeled HDL particles bind or help transport amyloid-related material in blood.
These mechanisms are plausible, but they are not proven.
The key point is that obicetrapib’s clearest biology is in the blood lipid system. The BROADWAY p-tau217 signal may reflect a downstream effect of that remodeling, but we do not yet know whether it is central, peripheral, vascular, HDL-mediated, or mixed.
What BROADWAY Tested
BROADWAY was a large cardiovascular lipid trial.
The parent trial evaluated obicetrapib in adults with established ASCVD, and/or heterozygous familial hypercholesterolemia. Participants were recruited from cardiology clinics and lipid specialty centers. They were already receiving maximally tolerated lipid-lowering therapy, but their LDL cholesterol remained inadequately controlled [1].
So BROADWAY did not enroll a general aging population. It enrolled people with residual lipid and cardiovascular risk.
The trial randomized 2,530 participants in a 2:1 ratio to obicetrapib 10 mg daily or placebo for 12 months. The parent trial’s main lipid readout was LDL-C lowering. At day 84, LDL-C decreased by about 30% with obicetrapib and increased slightly with placebo, producing a placebo-adjusted LDL-C difference of about 33%. Obicetrapib also increased HDL-C by more than 130% and lowered Lp(a) by about one-third [1].
The BROADWAY study materials summarize the key inclusion criteria as ASCVD or HeFH, LDL-C of at least 55 mg/dL with additional risk factors or LDL-C of at least 100 mg/dL, and maximally tolerated lipid-lowering therapy [1]. The parent trial endpoints included LDL-C at 12 weeks as the primary endpoint, with ApoB, Lp(a), non-HDL-C, and safety as key readouts [1].
That context is important.
The Alzheimer’s biomarker substudy did not arise from a general Alzheimer’s prevention cohort. It arose from a lipid-risk population, which may be exactly where a lipid-modifying drug is most likely to show a signal.
What the Biomarker Substudy Found
The Alzheimer’s biomarker analysis used stored blood samples from participants who had known APOE status and p-tau217 measured at baseline and after 12 months. The analysis included 1,535 of the 2,530 randomized BROADWAY participants, or 61% of the randomized population [1].
In the overall biomarker group, p-tau217 rose less in people who received obicetrapib than in people who received placebo. The signal appeared stronger in APOE4 carriers and strongest in APOE4/E4 participants.
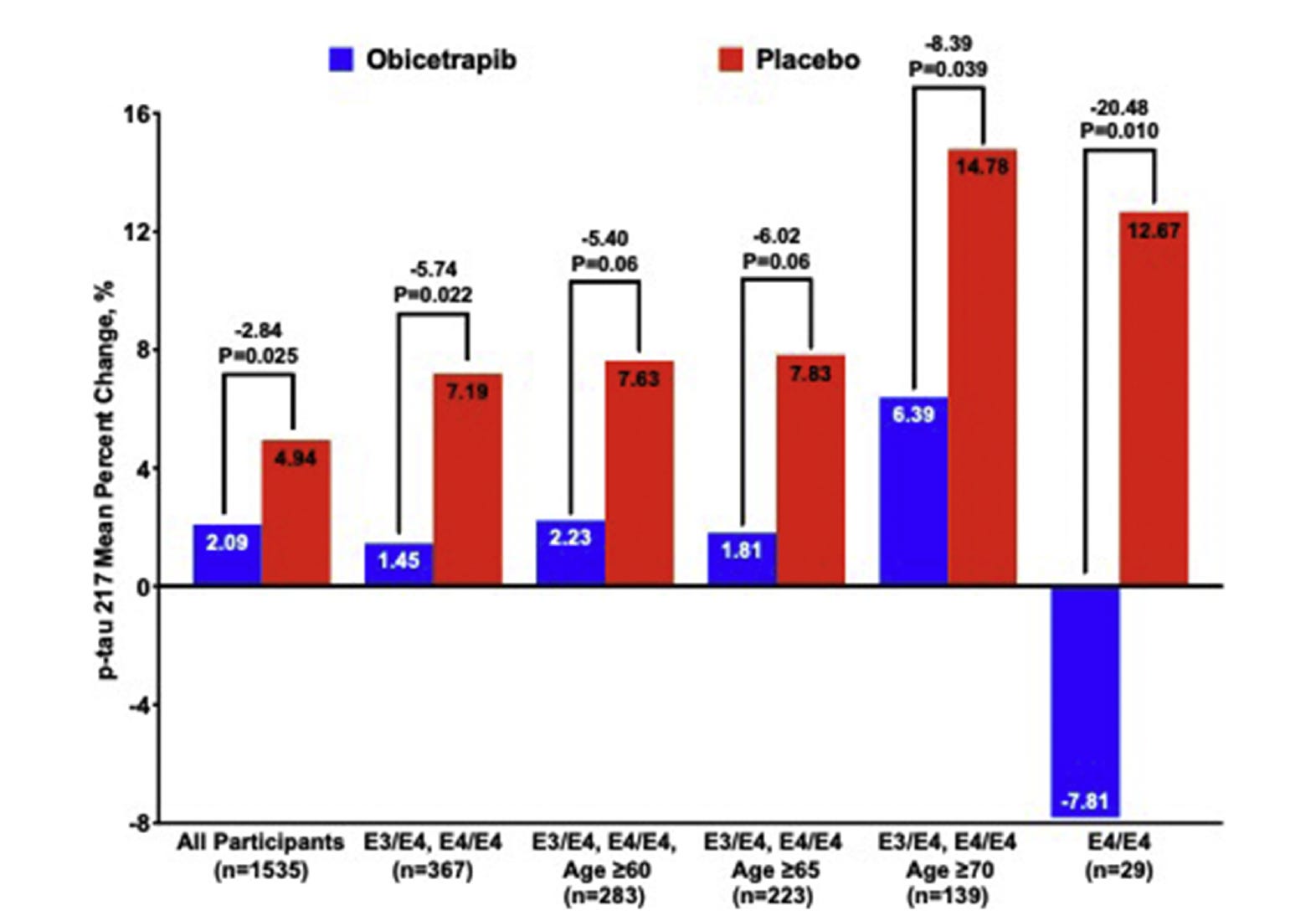
Among APOE4/E4 participants, p-tau217 decreased with obicetrapib and increased with placebo, producing a placebo-adjusted difference of about 20%. Other biomarkers also moved in a favorable direction in APOE4/E4 participants, including GFAP and NfL [1].
This is biologically interesting. It supports the idea that lipid modulation may affect Alzheimer’s-related biomarkers, especially in people with APOE4.
But the subgroup details are important.
Of the 1,535 participants in the biomarker analysis, 1,045 were APOE3/E3, 338 were APOE3/E4, 20 were APOE2/E4, and only 29 were APOE4/E4 [1].
That means the most striking APOE4/E4 finding came from a small subgroup.
Small subgroups can reveal real biology, but they can also produce unstable estimates. A large effect in 29 people is worth following, but it requires replication before it can carry the weight of any clinical claim.
The cardiovascular enrichment also matters. In the BROADWAY biomarker subset, most APOE4 carriers had established ASCVD because the parent trial required ASCVD and/or HeFH. From the subgroup table, approximately 87% of APOE4 carriers in the biomarker substudy had ASCVD. About 81% had hypertension, and about 38% had diabetes. Among APOE4/E4 participants specifically, about 86% had ASCVD, about 83% had hypertension, and about 45% had diabetes [1].
That is not a typical APOE4 prevention cohort.
BROADWAY’s APOE4 carriers were genetically at risk, but they were also heavily enriched for vascular and metabolic risk. That combination may be central to why the signal appeared.
How to Read the BROADWAY Analysis Fairly
The BROADWAY biomarker analysis has real strengths. It came from a randomized, double-blind, placebo-controlled parent trial. The Alzheimer’s biomarker analysis was pre-specified. The overall biomarker sample was substantial. The biological rationale is plausible. And the main p-tau217 finding is worth following.
A fair reading also requires caution.
First, this was a biomarker substudy of a cardiovascular lipid trial, not a dedicated Alzheimer’s prevention trial. It did not test whether obicetrapib slows memory decline, prevents mild cognitive impairment, or prevents dementia.
Second, the substudy examined many outcomes: p-tau217 overall, APOE subgroups, APOE4/E4 participants, age subgroups, p-tau217/Aβ42:40, GFAP, NfL, p-tau181, lipid correlations, and obicetrapib blood-level correlations. These analyses are useful, but the paper states that p values were not adjusted for multiplicity [1]. That means the pre-specified main biomarker result deserves the most weight, while subgroup and secondary biomarker findings are best treated as hypothesis-generating.
Third, a subgroup pattern is not the same as a formal interaction analysis. If the treatment effect looks larger in APOE4 carriers, that does not automatically prove that APOE genotype modifies treatment response. That requires a treatment-by-APOE interaction analysis. Without that, the careful statement is that the signal appeared stronger in APOE4 carriers, not that APOE4 has been proven to modify response.
Finally, baseline p-tau217 may matter. APOE4/E4 participants had higher p-tau217 at baseline, and the paper reported that participants with higher baseline p-tau217 appeared to show greater treatment effects [1]. That raises an important question: was the stronger APOE4/E4 signal due to APOE4 biology, higher baseline p-tau217, lipid risk, ASCVD, or some combination of all these factors?
That is the key precision-prevention question.
The best target population may not be APOE4 alone. It may be APOE4 plus elevated p-tau217 plus lipid dysfunction. Or it may be elevated Alzheimer’s biomarkers plus measurable lipid dysfunction, even without APOE4.
The Statin Lesson: LDL May Define the Responder
Statins provide a useful lesson for obicetrapib.
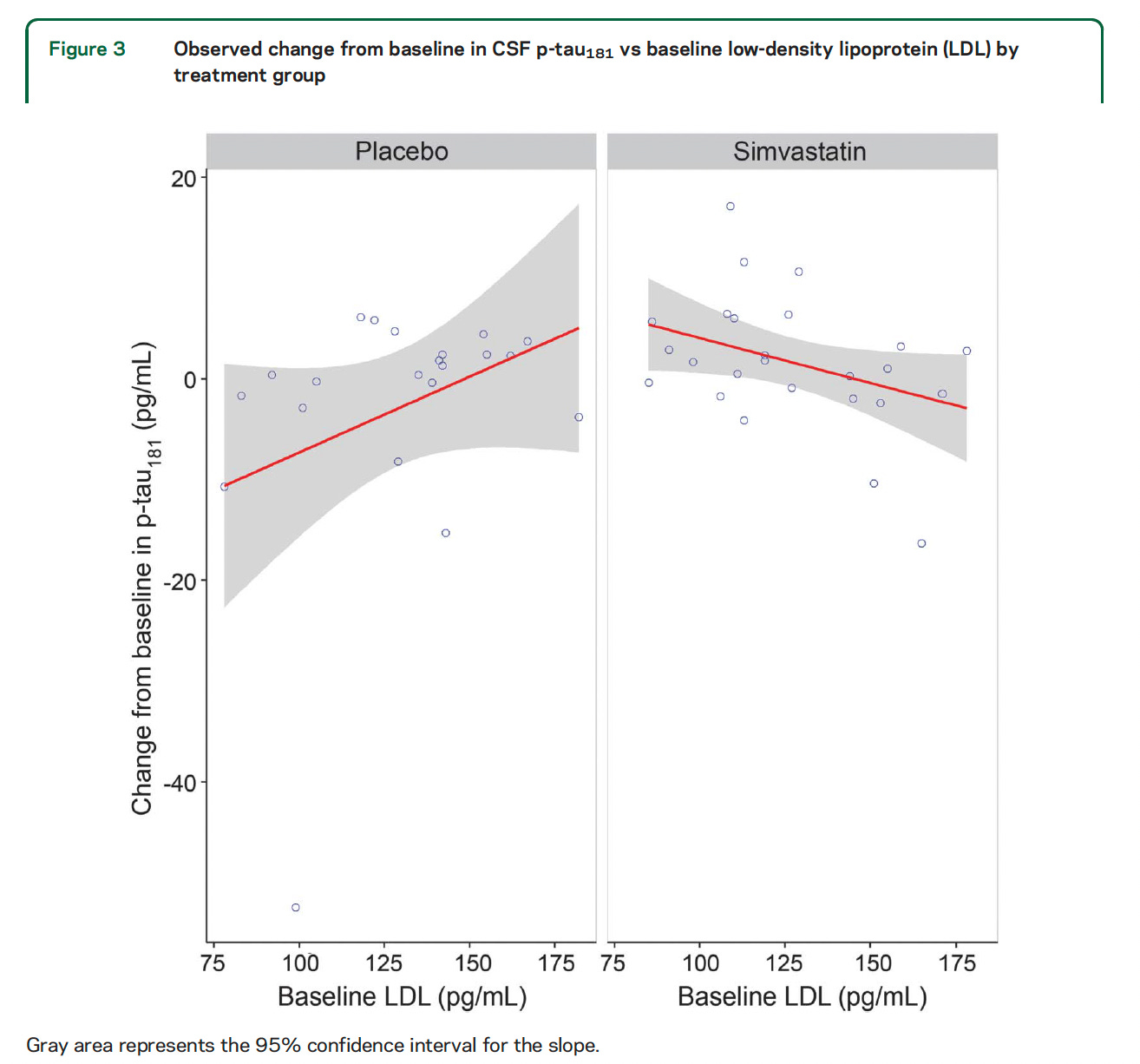
In a 12-month randomized, placebo-controlled trial, Li and colleagues tested simvastatin in cognitively normal adults. Participants were 45 to 64 years old, statin-naive, cognitively normal, and had normal or mildly elevated cholesterol. Forty-nine people were randomized, and 46 completed the study per protocol: 25 in the simvastatin group and 21 in the placebo group. Simvastatin was titrated to 40 mg per day. The primary outcomes were CSF Aβ42, total tau, and p-tau181 measured at baseline and after 12 months [2].
Overall, simvastatin did not significantly change CSF Aβ42, total tau, or p-tau181 compared with placebo. It also did not produce significant differences in neuropsychological test changes.
But the most informative result may have been hidden in the biology of the participants. Baseline LDL modified the treatment effect on CSF p-tau181. People with higher baseline LDL appeared to have greater reductions in CSF p-tau181 on simvastatin. The authors concluded that simvastatin-related reductions in CSF p-tau181 may be modulated by LDL cholesterol and merit further study in people with hypercholesterolemia [2].
That is directly relevant to obicetrapib.
A lipid-lowering drug may show its clearest brain biomarker effect in people whose lipid biology is abnormal. If a trial includes many people without elevated LDL, ApoB, Lp(a), or other lipid risk, the average effect may look smaller than it really is in the subgroup most likely to respond.
The lesson is not that statins prevent Alzheimer’s disease.
The lesson is that the responder population matters.
For obicetrapib, the key question may not be whether it works in all people with APOE4 or all people with elevated p-tau217. The more precise question is whether it works best in people with Alzheimer’s biology plus measurable lipid dysfunction.
The EVOKE Lesson: Biomarkers Need the Right Biology and the Right Outcome
EVOKE and EVOKE+ provide a second lesson.
These were large phase 3 trials of oral semaglutide in early Alzheimer’s disease, enrolling a combined 3,808 adults with early-stage Alzheimer’s symptoms and following participants for about two years [4].
The trials were important because GLP-1 receptor agonists have strong biological rationale. They improve metabolic health, insulin resistance, inflammation, vascular risk, and weight — pathways that may matter for brain aging.
The biomarker readout was encouraging. Semaglutide reduced several CSF biomarkers compared with placebo, including p-tau217 and other Alzheimer’s-related markers.
But the clinical readout was negative: semaglutide did not significantly slow disease progression compared with placebo [4].
This matters for two reasons.
First, it shows that moving Alzheimer’s biomarkers does not guarantee cognitive benefit.
Second, EVOKE was an Alzheimer’s disease trial, but it was not primarily designed around the metabolic phenotype where GLP-1 receptor agonists are most powerful. GLP-1 drugs often work best in people with obesity, insulin resistance, diabetes, cardiometabolic disease, or related inflammatory-metabolic risk. If those features are not central to trial enrichment, the average effect may dilute the benefit in the subgroup most likely to respond.
That is another lesson for obicetrapib.
Obicetrapib is a lipid-modifying drug. Its best test may require more than Alzheimer’s biomarkers or APOE genotype. It may require identifying the people whose Alzheimer’s risk is tied to lipid or vascular dysfunction.
In other words, the question is not only whether the drug can move p-tau217.
The question is whether the trial has selected the population most likely to benefit from the way the drug works.
The Mechanism Is Still Uncertain
There are several possible explanations for the BROADWAY p-tau217 signal.
It could be a central effect, meaning obicetrapib changes processes inside the brain. But we do not yet know whether obicetrapib enters the human brain in meaningful amounts.
It could be a vascular effect. BROADWAY participants had high cardiovascular risk, and obicetrapib improved lipid markers linked to vascular disease.
It could be an HDL-mediated peripheral effect. CETP inhibition may create larger or more functional HDL particles that improve cholesterol efflux, antioxidant defense, and inflammatory signaling.
It could also involve a peripheral sink effect, where remodeled HDL particles bind or transport amyloid-related proteins in blood, changing plasma biomarker dynamics without proving that tau pathology inside the brain has changed.
These possibilities are not mutually exclusive.
The next studies need to connect plasma p-tau217 to CSF biomarkers, amyloid PET, tau PET, vascular markers, HDL function, drug exposure, and cognition.
The key question is not only whether obicetrapib lowers p-tau217.
It is how it lowers p-tau217 — and whether that mechanism leads to clinical benefit.
APOE4, Lipids, and Trial Design
APOE4 makes obicetrapib interesting because APOE is a lipid transport gene.
In the brain, APOE helps move cholesterol and phospholipids between astrocytes, neurons, microglia, and other cells. These lipids are needed for synapses, membrane repair, myelin, and normal cellular signaling. APOE4 appears less efficient than APOE3 in several aspects of lipid handling and repair.
So it is plausible that some APOE4-related brain risk is mediated through lipid biology.
But APOE4 is not the same as a lipid phenotype.
Population studies show that APOE4 carriers, on average, have higher total cholesterol and LDL cholesterol than APOE3 carriers [6]. But averages do not define individuals. The percentage of APOE4 carriers with elevated LDL, low HDL, high ApoB, high Lp(a), metabolic syndrome, or ASCVD depends on the population being studied.
That matters for obicetrapib.
A trial enriched for APOE4, p-tau217, or GFAP may identify people at Alzheimer’s risk, but it may not identify the people most likely to respond to a lipid-modifying drug.
For obicetrapib, the most informative population may be people with both Alzheimer’s biology and lipid biology: APOE4 plus elevated p-tau217, high LDL-C or ApoB, elevated Lp(a), low HDL function, ASCVD, metabolic syndrome, or combinations of these factors.
The trial design should match how the drug works.
SPINOZA is coming next
The name SPINOZA also carries a useful meaning. Baruch Spinoza was a 17th-century Dutch philosopher whose work helped shape Western ideas about reason, nature, freedom, and the unity of mind and body. That connection is fitting here: the trial asks whether changing biology outside the brain — lipid metabolism in the blood and vasculature — might influence Alzheimer’s biology inside or around the brain.
SPINOZA is a phase 2b randomized, double-blind, placebo-controlled trial testing obicetrapib in people with preclinical Alzheimer’s disease. Unlike BROADWAY, it is designed around Alzheimer’s prevention rather than cardiovascular lipid lowering [5].
The primary endpoint is change in plasma p-tau217 at week 52. Secondary endpoints include Aβ42/40, p-tau217/Aβ42, p-tau217/Aβ42/40, p-tau181, and brain-derived tau. Cognition is exploratory and measured with the Preclinical Alzheimer Cognitive Composite 5, or PACC5 [5].
SPINOZA plans to enroll up to 400 participants, including at least 100 APOE4/E4 participants, plus 125–150 APOE3/E4 and 125–150 APOE3/E3 participants [5].
That is an important design. It prospectively tests the signal in a preclinical Alzheimer’s population and intentionally includes a larger APOE4/E4 group.
The key point is not to criticize SPINOZA before it starts. The key point is that its most informative analyses may depend on careful phenotyping.
Since obicetrapib is a lipid-modifying drug, the trial could be especially informative if it reports and analyzes LDL-C, ApoB, Lp(a), HDL-C, triglycerides, metabolic syndrome, diabetes, ASCVD, statin use, PCSK9 inhibitor use, baseline p-tau217, GFAP, and drug exposure.
Not all APOE4 carriers have high LDL, low HDL, high ApoB, high Lp(a), metabolic syndrome, or ASCVD. If many participants have preclinical Alzheimer’s biology but relatively normal lipid biology, the average treatment effect could be diluted.
That does not make the trial weak. It makes subgroup and interaction analyses essential.
For a lipid drug, the most informative trial design considers both Alzheimer’s biology and lipid biology.
Conclusion: From Signal to Reproducible Science
BROADWAY produced a promising p-tau217 signal. The signal appeared strongest in APOE4 carriers, especially APOE4/E4 participants. The finding is biologically plausible and deserves prospective testing.
But it should not be overstated.
BROADWAY does not prove that obicetrapib prevents Alzheimer’s disease. It does not prove that obicetrapib slows memory decline. It does not prove that APOE4 carriers, as a broad group, benefit more. And it does not tell us whether the p-tau217 effect is central, peripheral, or both.
What BROADWAY does is point to a serious hypothesis: lipid biology may be a modifiable pathway in Alzheimer’s prevention, especially in people with APOE4, vascular risk, lipid dysfunction, and elevated Alzheimer’s biomarkers.
That is an important hypothesis.
Now it needs reproducible testing.
The next studies could select participants based on biology, test APOE interactions directly, test lipid interactions directly, measure biomarkers carefully, include cognitive outcomes, follow people long enough, and avoid turning subgroup findings into clinical claims before they are reproduced.
The main lesson is that Alzheimer’s prevention trials need to match the drug to the biology it is designed to modify.
For obicetrapib, that biology is lipid metabolism.
The right conclusion is not:
“Obicetrapib prevents Alzheimer’s disease.”
The right conclusion is:
“Obicetrapib produced a promising lipid-biology signal that now needs rigorous prospective testing in the right biological population.”
That is how reproducible prevention science can move forward.
Take-Home Messages
Trial context matters. BROADWAY was a cardiovascular lipid trial, not a dedicated Alzheimer’s prevention trial.
Mechanism matters. Obicetrapib’s clearest biology is peripheral lipid remodeling.
Subgroups need discipline. The APOE4/E4 signal is promising, but the subgroup was small and needs interaction testing and replication.
Biomarkers are not cognition. EVOKE and EVOKE+ showed that p-tau217 and other CSF biomarkers can improve without clinical benefit.
APOE4 is not a lipid phenotype. The most informative population may be people with Alzheimer’s biology plus measurable lipid or vascular dysfunction.
The mechanism remains open. The p-tau217 effect could be central, vascular, peripheral, HDL-mediated, or mixed.
Precision prevention means matching the drug to the biology and the responder population. Obicetrapib acts on lipid metabolism, so the most informative trials may be those that identify people whose Alzheimer’s risk is tied to lipid or vascular dysfunction, not only APOE genotype or p-tau status.
Relevant Disclosure:
I sit on the advisory board of New Amsterdam Pharma, which is developing Obicetrapib
References
Davidson MH, Szarek M, Scheltens P, et al. Effect of obicetrapib, a potent cholesteryl ester transfer protein inhibitor, on p-tau217 levels in patients with cardiovascular disease. Journal of Prevention of Alzheimer’s Disease. 2025. doi:10.1016/j.tjpad.2025.100394.
Li G, Mayer CL, Morelli D, et al. Effect of simvastatin on CSF Alzheimer disease biomarkers in cognitively normal adults. Neurology. 2017;89:1251–1255.
Corcoran E, Kettlety M, Mogul U, Azah JN, Cork SC. The effects of GLP-1 receptor agonists on Alzheimer’s pathophysiology: a systematic review. Molecular and Cellular Neuroscience. 2026;137:104091.
Novo Nordisk. Headline results from the EVOKE and EVOKE+ phase 3 trials of oral semaglutide in early Alzheimer’s disease. Reported 2025.
SPINOZA Study. A Phase 2b, randomized, double-blind, placebo-controlled, parallel group study to assess the efficacy and safety of obicetrapib in participants with preclinical Alzheimer’s disease. Protocol Synopsis Version 1.0, 01 Apr 2026.
Bennet AM, Di Angelantonio E, Ye Z, et al. Association of apolipoprotein E genotypes with lipid levels and coronary risk. JAMA. 2007;298(11):1300–1311.
Alberti KGMM, Eckel RH, Grundy SM, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640–1645.