

A Reading of the MIND, FINGER, and US POINTER lifestyle interventions for AD
Progress, Missed Opportunities and Why Lifestyle Trials for Alzheimer’s Are So Hard to Get Right

Every few years, a new headline promises that diet or exercise can protect the aging brain. The observational evidence is encouraging: people who eat well, move regularly, and stay socially engaged tend to have lower rates of dementia. But turning that association into a randomized trial that proves cause and effect — and honestly communicating what the trial found — has been one of the most fraught exercises in modern neuroscience. Two trials, FINGER, and the newly reported U.S. POINTER, are usually cited as the field’s biggest wins. Looked at closely, the real story is more about who was studied and what they were compared against than about an “optimizing lifestyle” program to prevent dementia.
Finding the right population
The first problem for lifestyle trials is deciding who to enroll. Enroll people already impaired, and you’re fighting neurodegeneration built up over a decade. Enroll young and healthy people, and you may need twenty years before enough develop dementia to measure anything. FINGER recruited adults aged 60–77 with an elevated CAIDE dementia risk score (vascular risk factor score) and cognition at or just below what’s expected for their age [1]. U.S. POINTER cast a wider net: about 2,100 older adults, 78% with a family history of memory loss and 30% carrying the APOE-e4 gene copy, recruited to include groups historically underrepresented in dementia research [2]. MIND enrolled people with a family history of dementia, a BMI over 25, and — this is worth being precise about — a MIND diet screener score of 8 or less out of 14, meaning eligibility required eating poorly by that specific measure [3]. That’s a genuinely hard recruitment target, and credit is due for the effort: of roughly 1,900 people screened, more than 500 were excluded for already eating too well on the MIND scale. This was not a casual “self-reported suboptimal diet” — investigators actively went looking for a diet-deficient population.
There’s a further wrinkle worth naming, though: advantaged and diet-poor are not the same thing. FINGER and POINTER recruited educated, engaged older adults with reasonable baseline access to exercise, social stimulation, and health care — capable of sustaining a multi-year program. MIND, despite deliberately selecting for a poor baseline diet, still enrolled a demographically similar cohort on nearly every other axis: 87.7% white and an average of 16.9 years of education, recruited through two academic medical centers. A low MIND-diet score and genuine socioeconomic disadvantage are different problems, and it’s easy to conflate them. Layering an elaborate program onto an already-favorable baseline — of education, health-system access, and time to participate — has a much smaller ceiling to push against than aiming the same idea at a population without stable food access, safe places to exercise, or equivalent support.
That reframes where the bigger opportunity might sit. A far cheaper intervention — reliable access to real food, a free community fitness membership, social infrastructure as a safety net — delivered to a population currently missing all of that could plausibly produce a larger absolute effect than an elaborate protocol layered onto people already doing reasonably well.
The FINGER investigators noticed this population gap. World-Wide FINGERS has expanded to more than 40 countries, including Africa-FINGERS, now piloting structured multidomain coaching across several African nations with genuine community co-design [4]. But what’s being exported is still the FINGER template — coached diet counseling, structured exercise, cognitive training, vascular monitoring — adapted in delivery, not in kind. A different, more urgent question: does closing the gap itself — food security, safe places to exercise, a functioning safety net — produce more benefit, more cheaply, than a coached protocol layered on scarcity? That trial, as far as I can tell, hasn’t been run.
None of that is meant to sound easy. Recruiting and retaining a genuinely underserved population in a multi-year lifestyle trial is its own serious problem — transportation, work schedules, trust in research institutions, and the competing demands of poverty all erode compliance in ways a motivated, retired, academic-medical-center-adjacent volunteer pool doesn’t face. That’s precisely why a standard multi-year RCT of the FINGER or POINTER kind may be the wrong instrument here. Pragmatic and decentralized trial designs — community-embedded cluster randomization through existing food-assistance or primary-care infrastructure, stepped-wedge rollouts, or remote and digital monitoring that cuts down on repeated clinic visits — are better suited to testing a basic-access intervention in a population a conventional trial would struggle to retain.
Choosing the intervention — and the control
FINGER and POINTER both bundled diet, exercise, cognitive training, and vascular risk management together. MIND isolated one variable, testing a hybrid Mediterranean-DASH diet against a mild-calorie-restriction control [3]. But the more revealing design choice, across all three, is what the comparison group actually received — and in every case, it wasn’t nothing. FINGER’s control got “regular health advice” on diet, exercise, and vascular risk. POINTER’s self-guided arm attended six peer group meetings, got general health education across every domain, and received small incentives [2]. MIND’s control diet produced almost exactly as much weight loss as the MIND diet itself — about five kilograms in both arms over three years, with real protective effects on blood pressure, lipids, and insulin sensitivity baked into both arms before the specific food pattern is even considered.
MIND’s design raises a further question, and it’s baked into the score itself, not just the intervention. The MIND diet index sums 15 food groups — 10 to eat more of (leafy greens, other vegetables, nuts, berries, beans, whole grains, fish, poultry, olive oil, wine) and 5 to eat less of (red meat, butter, cheese, pastries and sweets, fried food). It’s an optimization checklist, built to reward a specific idealized eating pattern, not a measure targeted at ultra-processed food intake, added sugar, or fiber as such. Someone can score low on MIND simply by skipping berries, nuts, and olive oil, whether or not their diet is high in ultra-processed food; someone else could hit enough of the positive categories to score reasonably while still eating a lot of packaged, sugar-heavy, low-fiber food the index was never built to catch. The typical U.S. diet MIND’s participants started from derives roughly 55% of calories from ultra-processed foods [5], and both low fiber and high ultra-processed intake are independently linked to worse cognitive trajectories via gut-brain and inflammatory pathways [6,7] — pathways the MIND score, by design, wasn’t built to target directly. Cutting calories, ultra-processed foods, and raising fiber may be the bigger lever than a curated food list of berries, olive oil, and nuts layered on a diet still built around what it should avoid.
That matters for how to read the results. The real question isn’t “does lifestyle change help, compared with nothing.” It’s narrower: does an intensive, expert-coached optimization protocol add much on top of the active ingredient the comparison group already shared — guidance in FINGER, structured support in POINTER, weight loss in MIND? In all three, the honest answer is: a little, but not a lot — a very different message than “breakthrough lifestyle program prevents cognitive decline,” which is closer to how these trials were actually presented.
Reading the effect sizes honestly
This is where the field’s self-presentation runs ahead of the data. FINGER’s primary outcome, a composite neuropsychological z-score, improved 0.20 in the intervention group and 0.16 in control over two years [1] — an absolute difference of about 0.04 standard deviations (see illustration below). Reported as “25% greater improvement than control,” that’s true, but it’s a relative figure built on a very small absolute one, and the same arithmetic produced the widely quoted 83% gain in executive function and 150% gain in processing speed.
A more honest yardstick is Cohen’s d, the standard way to express an effect on a common scale, alongside its plain-language twin, the common language effect size: the odds a random person from the structured group scored higher than a random person from the comparison group. Using FINGER’s own model-based d ≈ 0.13, that’s roughly a 54-in-100 chance — barely better than a coin flip. Given the comparison group wasn’t null but a lighter-touch version of the same idea, that’s about what you’d expect: the marginal value of intensive structuring on top of ordinary guidance, not lifestyle change measured against nothing. (This figure comes from the trial’s own supplementary analyses; check the appendix directly.)
What’s notable is less the size of that number than how it’s been communicated: as a landmark breakthrough, driving funding to replicate the FINGER model in more than 60 countries through World-Wide FINGERS. A modest, real, worth-pursuing signal is not a breakthrough.
U.S. POINTER’s own translation — “equivalent to one to two years of slowed cognitive aging” — deserves similar scrutiny. That figure is a model-based extrapolation against an assumed normative decline rate, not a directly observed outcome — a generous way to make a small number sound tangible. It’s worth knowing this framing appears prominently in Alzheimer’s Association press materials; the Association is also a funder, which doesn’t make the number wrong, but is reason to read it as favorable communication rather than a hard result.
Set against the wider record, FINGER and POINTER look like the best case, not the norm. MAPT [8] found no significant effect on cognitive decline; preDIVA [9] — the rare trial actually powered to detect a difference in dementia incidence itself — found none either; nor did HATICE [10] (see table below). “Mixed and modest” is a fair summary of this literature.
preDIVA’s null result also points to a structural problem: incident dementia is an extraordinarily hard outcome to power a trial on, requiring thousands of participants and years of follow-up — why most trials fall back on cognitive composites as a proxy, the very proxies producing the small, hard-to-interpret effect sizes above. This is a core reason nutrition and lifestyle trials are structurally harder to design than drug trials: drugs can often show a biomarker signal, while lifestyle change needs years before it plausibly shows up in diagnosable disease.
Effect sizes across the major prevention trials, at a glance:
Trial Comparison Primary effect size Plain-language interpretation FINGER (2015) [1] Coaching vs. general health advice, 2 yrs Composite z: 0.20 vs 0.16 (Δ≈0.04 SD); d ≈ 0.13 ~54-in-100 chance a treated person outscores a control person — barely above a coin flip U.S. POINTER (2025) [2] Structured vs. self-guided coaching, 2 yrs 0.029 SD/yr greater, structured arm Marketed as “1–2 years of slowed cognitive aging” — a model-based extrapolation, not a measured outcome MIND (2023) [3] Diet vs. calorie-restriction control, 3 yrs No significant difference in cognition or MRI Both arms improved and lost ~5 kg; weight loss, not the food pattern, may be the active ingredient MAPT (2017) [8] Coaching + omega-3 vs. placebo, 3 yrs No significant effect on cognitive decline Null on the primary outcome preDIVA (2016) [9] Nurse-led vascular care vs. usual care, 6 yrs Dementia incidence: 7% vs 7%; HR 0.92 Null; the rare trial actually powered on dementia diagnosis, not a proxy HATICE (2019) [10] Internet-coached vascular care vs. control, 18 mo No significant cognitive effect Modest improvement in cardiovascular risk factors only
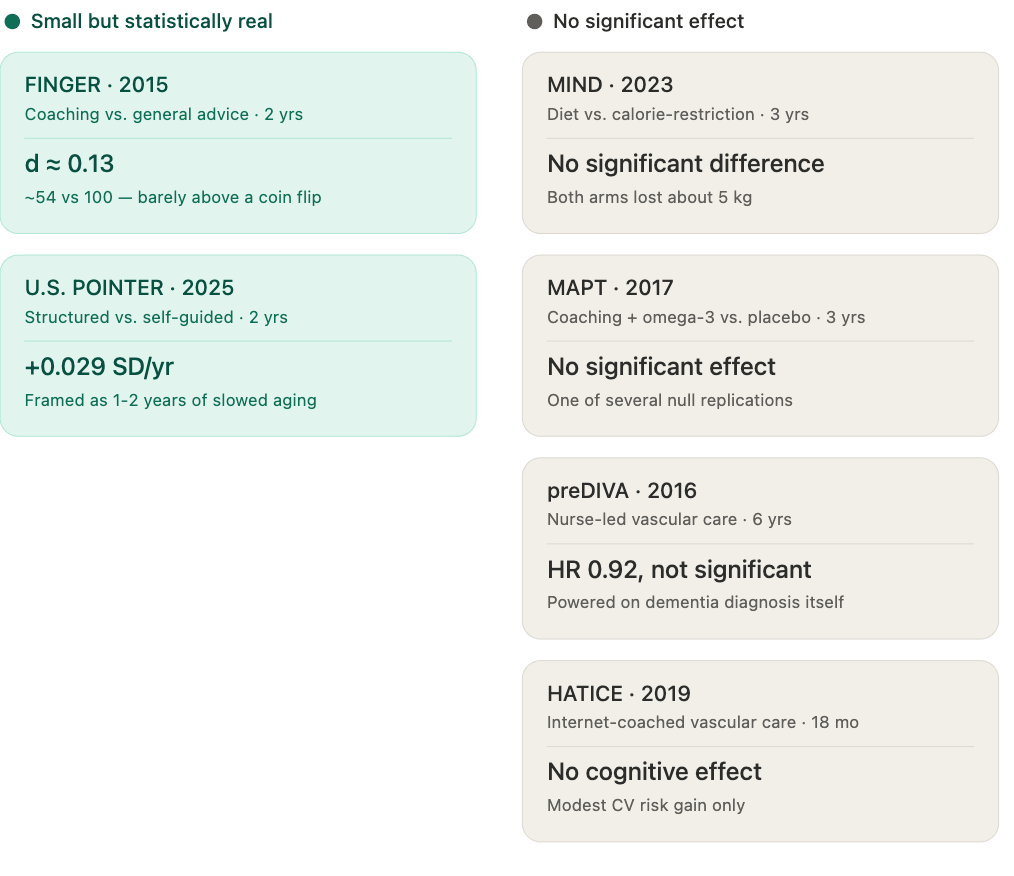
The two columns look like a verdict — "significant" versus "null" — but the underlying effect sizes are small enough on both sides that the line between them is closer to a statistical threshold than a true difference in what these interventions accomplished. A slightly larger sample, or a slightly different outcome measure, could plausibly have moved several of these trials across the line in either direction.
Choosing outcomes that match the mechanism
Layered on the incidence problem is a measurement problem, and it isn’t just that standard batteries are blunt — they may be tuned to the wrong domain. Look again at FINGER’s own breakdown by cognitive domain: the largest relative gains were in executive function (83%) and processing speed (150%), while memory — the domain most closely tied to classic Alzheimer’s pathology, and the one nearly every AD drug trial is built around — showed the smallest relative gain, at 40%. That pattern fits what a lifestyle intervention plausibly does: support attention, task-switching, and processing speed through cardiovascular and metabolic pathways, rather than directly reversing amyloid-and-tau-driven memory decline.
Standard batteries, though, are built around exactly the domain lifestyle interventions seem to move least. Memory subtests dominate most AD-oriented composites, because memory is what clinicians use to diagnose dementia. Executive function and processing speed are typically assessed with a handful of brief, coarse paper-and-pencil tasks — a few minutes of Trail Making or digit-symbol substitution — far less sensitive to subtle change than a memory test built and validated for detecting AD. If the domains most responsive to diet and exercise are the ones our batteries measure worst, that could make a real effect look smaller and noisier than it is, on top of the floor, ceiling, and practice effects already limiting these tools in healthy populations [11,12].
This is where digital assessment tools have a genuine edge, beyond being reliable or convenient. They can deliver dozens of processing-speed and executive-function trials in a single sitting, repeated over months from a phone, with millisecond-level precision a stopwatch and paper form can’t match — capturing graded change in reaction time and task-switching cost, not one coarse pass-fail score. Repeated at-home testing also averages out day-to-day noise and practice-effect drift, which often swamps small true effects in one-off batteries. A recent scoping review found digital tools improve reliability and ecological validity relative to a single in-clinic assessment [13]; the sharper opportunity is fitting the tool to the domain — fine-grained, repeatable measures of processing speed and executive function as primary outcomes, rather than composite scores weighted toward a memory domain a diet-and-exercise program was never especially likely to move.
What basic science suggests we might be missing
A newly published mouse study adds a mechanistic layer here, not because mouse data settle anything about human trials, but because it shows how cell-type-restricted an exercise response can be. Researchers used single-nucleus RNA sequencing to identify which brain cells respond to exercise in the hippocampal dentate gyrus of an Alzheimer’s mouse model [14]. The response was concentrated in immature neurons, in a neurovascular-associated astrocyte population depleted in Alzheimer’s mice but partly restored by exercise, and in oligodendrocyte progenitor cells, which had the largest share of disease-related genes normalized by exercise of any cell type studied. An earlier study similarly found that long-term voluntary exercise reversed cognitive impairment in an Alzheimer’s mouse model through astrocyte remodeling, without changing amyloid-beta plaque burden [15]. Exercise may not clear the disease’s hallmark pathology so much as build a parallel, cell-specific form of resilience around it.
The clearest thread connecting these findings to the human domain pattern above runs through the neurovasculature unit. Both studies converge on astrocytes, cells that couple neural activity to blood flow and glucose delivery — so an exercise-induced astrocyte response plausibly improves neurovascular efficiency rather than clearing amyloid or tau directly. That fits a well-established pattern in the vascular cognitive impairment literature: circuits depending on blood flow and white-matter integrity, largely underlying processing speed and executive function, are especially sensitive to vascular health, while memory decline is more specifically driven by amyloid and tau damage to hippocampal circuits. If exercise, weight loss, and vascular risk management work substantially through this route, that would explain why FINGER’s and POINTER’s clearest signal was in executive function and processing speed, not memory — a coherent hypothesis, not a demonstrated mechanism, but better-specified than “lifestyle helps the brain.”
Uncertainty and future directions
None of this is settled. The cell-specific effects above come from mice, and the neurovascular story linking them to the human executive-function signal is a plausible synthesis, not a demonstrated chain. Real, useful signals are also getting inflated by relative-risk framing and normative-decline translations, in a field where funding rewards breakthrough narratives over careful ones — not reason to dismiss FINGER or POINTER, but reason to ask, as Africa-FINGERS scales up, whether it’s testing the right thing: an elaborate coached protocol exported wholesale, or a cheaper, gap-filling alternative that hasn’t had its own trial.
Take-Home Messages
Target the population where the room to improve is largest: FINGER, POINTER, and even diet-screened MIND enrolled cohorts that were educated and well-resourced, whatever their baseline diet score. A poor diet score and genuine socioeconomic disadvantage are not the same thing — the bigger opportunity likely sits in vulnerable populations with limited access to whole foods or exercise infrastructure, and even Africa-FINGERS is still exporting the expensive coached protocol rather than testing whether closing basic gaps works better alone.
De-emphasize expensive “optimization protocols”: every comparison group already received an active ingredient — health advice, self-guided coaching, or weight loss — and the elaborate add-on produced only a small increment on top. The MIND diet score itself is an optimization checklist, not a measure built around ultra-processed food, added sugar, or fiber; cutting ultra-processed foods and raising fiber may matter more than a curated food list.
Recruiting underserved populations is genuinely hard, and that’s not a footnote: transportation, work schedules, and trust in research institutions all erode compliance. Pragmatic, decentralized, or community-embedded trial designs may be better suited to testing basic-access interventions than a standard multi-year RCT.
Matching outcomes to mechanism: interventions working through vascular pathways plausibly act on processing speed and executive function more than on amyloid/tau-driven memory decline — outcomes should be weighted accordingly, not defaulted to memory-heavy composites built for drug trials.
Digital, phone-based executive-function testing could change the landscape: repeated, low-burden testing averages out day-to-day noise and practice effects, detecting small, domain-specific effects one-off batteries are too noisy to catch.
References
Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255-2263.
Baker LD, Espeland MA, Whitmer RA, et al. Structured vs self-guided multidomain lifestyle interventions for global cognitive function: the U.S. POINTER randomized clinical trial. JAMA. Published online July 28, 2025. doi:10.1001/jama.2025.12923.
Barnes LL, Dhana K, Liu X, et al. Trial of the MIND diet for prevention of cognitive decline in older persons. N Engl J Med. 2023;389(7):602-611.
Udeh-Momoh CT, Maina R, Anazodo UC, et al. Dementia risk reduction in the African context: multi-national implementation of multimodal strategies to promote healthy brain aging in Africa (the Africa-FINGERS project). Alzheimers Dement. 2024;20(suppl 12). doi:10.1002/alz.14344.
National Center for Health Statistics (CDC). Ultra-processed food consumption among adults and youth, United States, August 2021–August 2023. NCHS Data Brief No. 536. Hyattsville, MD: 2025.
Zhao Y, Bazan NG. Nutrition and gut-brain axis: opposing effects of dietary fiber and Western-style diets on Alzheimer’s disease. Curr Opin Clin Nutr Metab Care. 2026;29(4):421-430.
Gomes Gonçalves N, Vidal Ferreira N, Khandpur N, et al. Association between consumption of ultraprocessed foods and cognitive decline. JAMA Neurol. 2023;80(2):142-150.
Andrieu S, Guyonnet S, Coley N, et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 2017;16(5):377-389.
Moll van Charante EP, Richard E, Eurelings LS, et al. Effectiveness of a 6-year multidomain vascular care intervention to prevent dementia (preDIVA): a cluster-randomised controlled trial. Lancet. 2016;388(10046):797-805.
Richard E, Van den Heuvel E, Moll van Charante EP, et al. Healthy ageing through internet counselling in the elderly (HATICE): a multinational, randomised controlled trial. Lancet Digit Health. 2019;1(8):e424-e434.
Cohen S, Cummings J, Knox S, Potashman M, Harrison J. Clinical trial endpoints and their clinical meaningfulness in early stages of Alzheimer’s disease. J Prev Alzheimers Dis. 2022;9(3):507-522.
Aschenbrenner AJ, Hassenstab J, Wang G, et al. Avoid or embrace? Practice effects in Alzheimer’s disease prevention trials. Front Aging Neurosci. 2022;14:883131.
Berron D, et al. A scoping review of remote and unsupervised digital cognitive assessments in preclinical Alzheimer’s disease. npj Digit Med. 2025;8:266.
da Rocha JF, Lance ML, Luo R, et al. Protective exercise responses in the dentate gyrus of Alzheimer’s disease mouse model revealed with single-nucleus RNA-sequencing. Nat Neurosci. 2025;28:1546-1561.
Belaya I, Ivanova M, Sorvari A, et al. Astrocyte remodeling in the beneficial effects of long-term voluntary exercise in Alzheimer’s disease. J Neuroinflammation. 2020;17:271.